Use this link to enable the ReciteMe accessibility toolkit

The Code of Governance for NHS Provider Trusts 2022 (NHS Code) requires the division of responsibilities for the Chair, Chief Executive, Senior Independent Director, the Board and its committees to be set out in writing, agreed by the Board of Directors and made publicly available.
The NHS Code also states that ‘responsibilities should be clearly divided between the leadership of the board’ and that ‘no individual should have unfettered powers of decision’. As the Trust seeks to adhere to the NHS Code, these responsibilities have been set out in this statement.
The Board of Directors are responsible for setting the overall strategic direction of the trust. The business of the trust is managed by the Board of Directors, with all powers exercised by the Board of Directors on its behalf. The matters reserved for the Board of Directors and those delegated to individual directors or committees, are clearly documented within the Scheme of Delegation.
The Board operates in accordance with the Standing Orders and Reservations of Power and the organisation operates in accordance with the financial rules set out in the Standing Financial Instructions, agreed by the Board.
The Board has established committees to have oversight and seek assurance in specified areas. All committees have clear terms of reference that set out the scope of the committee’s responsibilities and any delegated powers from the Board. These committees report back to the Board after each meeting, providing assurance or escalating risks as appropriate.
The Chair is responsible for:
Board of Directors
Directors
Induction, development and performance evaluation
Governance
Role of the Chief Executive
Within the authority limits delegated by the Board, and not to the exclusion of any duty detailed in the Accounting Officer Memorandum, the Chief Executive is responsible for:
Business Strategy and Management
Investment and Financing
Risk Management and Controls
Board Committees
Communication
Human Resources
Responsibilities of the Senior Independent Director
The Board of Directors appoint one of the independent Non-Executive Directors to be the Senior Independent Director. The role of the Senior Independent Director is to:
This statement was approved by the Board of Directors at its meeting on 24 September 2025
JULIA MULLIGAN
Chair
For and on behalf of the Board of Directors
The Patient Safety Incident Response Framework (PSIRF) sets out the NHS’s approach to developing and maintaining effective systems and processes for responding to patient safety events, for the purpose of learning and improvement. Patient safety events are unintended or unexpected events (including omissions) in healthcare that could have, or did, harm one or more patients.
The PSIRF replaces the Serious Incident Framework (SIF), (2015) and makes no distinction between “patient safety events” and “serious incidents”. It removes the “serious incidents” classification and the threshold for it. Instead, the PSIRF promotes a proportionate approach to responding to patient safety events by ensuring resources allocated to learning are balanced with those needed to deliver improvement.
The new framework is not a different way of describing what came before; it fundamentally changes how the NHS responds to patient safety events for learning and improvement.
The PSIRF advocates a co-ordinated and data-driven approach to patient safety responses that prioritises compassionate engagement with those affected, including staff. It embeds a wider system of improvement and prompts significant cultural shift towards patient safety management.
This policy supports the requirements of the PSIRF and sets out North West Ambulance Service NHS Trust’s (NWAS) approach to developing and maintaining effective systems and processes for responding to patient safety events and issues for the purpose of learning and improving patient safety. This policy supports the four key aims of the framework:
This policy is specific to patient safety event responses conducted solely for the purpose of learning and improvement across NWAS. Responses under this policy follow a systems-based approach. This recognises that patient safety is an emergent property of the healthcare system: that is, safety is provided by interactions between components and not from a single component. Responses do not take a “person focused” approach where the actions or inactions of people, or “human error”, are stated as the cause of an event.
There is no remit to apportion blame or determine liability, preventability, or cause of death in a response conducted for the purpose of learning and improvement. Other processes exist for that purpose, and therefore outside of the scope of this policy, such as:
For clarity, the principle aims of each of these responses differ from those of a patient safety response and are outside the scope of this policy. Information can be shared with those leading other responses, but these processes should not influence the remit of a patient safety learning response.
NWAS is committed to work towards the move from a retribution approach to types of incidents, such as patient safety, to establishing a just culture within the organisation. Leaders across NWAS are required to proactively embrace this approach and support from staff side colleagues will be instrumental in supporting the organisation transition to a just culture.
The goals of just culture include:
PSIRF will enhance these by creating stronger links between patient safety events and learning for improvement. NWAS anticipates fostering the approach and work collaboratively with those affected including patients and their families, and our people. This will continue to increase transparency and openness amongst our people to report events and allow for wider engagement.
We are clear that patient safety event responses are conducted for the sole purpose of learning and identifying system wide improvements; they are not to apportion blame, liability or define preventability or cause of death.
Our safety culture within NWAS continues to make progress and is a key organisation priority. We have programmes of work in place to improve this including:
The Patient Safety Partner (PSP) role is a new and evolving role developed by NHS England to help improve patient safety across the NHS. At NWAS, we’re excited to welcome PSPs who will offer support alongside our people, patients, families, and carers to influence and improve safety across our range of services.
PSPs can be patients, carers, family members or other lay people (including NHS staff from another organisation) and offers great opportunities to share experiences and skills and provide a level of scrutiny. This exciting new role will evolve over time with the main purpose of the role is to be the voice for our patients and community who utilise our services, ensuring patient safety is at the forefront of all that we do.
PSPs will provide objective feedback focusing on maintaining safety and improvement. This may include attendance at our patient safety and quality governance meetings and involvement with the production and review of relatable policies and procedures. The information may be complex, and partners will provide feedback to ensure patient safety is our priority. PSPs will be supported in their honorary role by the Safety Learning Team and Patient Experience Team who will provide expectations and guidance for the role. They will have regular reviews and training needs will be agreed together, based on the experience and knowledge of each partner.
The PSP role will be reviewed annually to ensure the role is aligned to the patient safety agenda as it continues to develop, and expanded to ensure we are represented by the diverse communities we serve, including population groups who may sometimes experience challenges in accessing our services.
The NHS has a duty to reduce inequalities in health by improving access to services and tailoring those around the needs of the local population in an inclusive way.
The Trust is committed to delivering on its statutory obligations under the Equality Act, (2010) and will use data intelligently to assess any disproportionate patient safety risk to patients from across the range of protected characteristics. This data can be captured via our Electronic Patient Records (EPR) and DCIQ system.
In our response toolkit, we will directly address any features of an event which indicate health inequalities, that may have contributed to harm or demonstrate an ongoing risk to any population group, including all protected characteristics. When constructing safety improvement actions in our patient safety learning responses we will consider inequalities.
We will look to address health inequalities as part of our safety improvement work, understanding our services provide care to a proportion of the Core20PLUS5 population cohort identified by NHS England (2021). In establishing our future policy and plan we will work to identify variations of inequality by using our population and patient safety data to ensure it is considered as part of the development process for the future.
Engagement of those involved (patients, families/carers, and our people) following a patient safety event is crucial to our patient safety learning responses. We will ensure that we use available tools to include easy read, translation, and interpretation services alongside any other method appropriate to meet their needs and maximise the potential of being involved.
Information resources produced by NWAS can be made available in alternative formats, such as easy read or large print and may be available in alternatives languages upon request. These requests can be made to our internal communications team.
NWAS endorses a zero tolerance of racism, discrimination, and unacceptable behaviours from and towards our people, our patients, carers, and families.
PSIRF recognises that learning and improvement following a patient safety event can only be achieved if supportive systems and processes are in place. It supports the development of an effective patient safety response system that prioritises compassionate engagement and involvement of those affected. This involves working with those affected to understand and answer any questions in relation to the event and signpost to relevant support as required.
We are committed to continuous improvement throughout the services we provide. We want to learn from any event where care does not go as planned or expected by our people, patients, their families, carers, and other organisations. Getting involvement right with patients and families in our response is crucial, particularly to support the improvement of the services we provide. This involves being open and honest whenever there is a concern about care/ treatment provided, or when a mistake has been made.
Alongside professional and statutory requirements for Duty of Candour, NWAS commits to being open and transparent because it’s the right thing to do; this is regardless of the level of harm caused by an event. In-line with the PSIRF we will support those involved via a network of Engagement Leads who will guide our people, patients, and their families through our patient safety learning responses to conclusion.
In addition, we have a Patient Advice and Liaison Service (PALS) for those with a concern or are unhappy about their experience with NWAS. This allows the organisation to review the concern and make improvements where necessary and feasible.
NWAS loves to hear great things about our people and the services we provide and NWAS welcomes compliments from our patients and their families which are used to assist with learning from excellence.
Our teams at NWAS can support with the following:
All relevant contact details and associated forms can be found on our contact us page.
For our people, NWAS recognises it can be beneficial to seek support because of a patient safety event they have been involved in and NWAS advocates the equal importance of both mental and physical health. Our people are encouraged to access the dedicated ‘Invest in Yourself’ webpage where there are a range of guides and supportive resources.
Patients/ families and carers may find support from one of the following sources: (please note this is not an exhaustive list).
PSIRF supports organisations to respond to patient safety events and issues in a way that maximises learning and improvement, rather than basing responses on arbitrary and subjective definitions of harm. Beyond nationally set requirements, we can explore patient safety events relevant to their context and the populations we serve rather than only those meeting a defined threshold.
NWAS will take a proportionate approach to its response to patient safety events, ensuring the focus is on maximising improvement. To fulfil this, we will proactively undertake planning of our current resources for patient safety learning response and our existing safety improvement workstreams.
Our Patient Safety Incident Response Plan (PSIRP) will detail how this will be achieved alongside how we intend to meet both National requirements and our NWAS Local Priorities for patient safety incident responses.
NWAS has committed to ensuring that we fully embed PSIRF and meet the national training requirements. We have utilised NHS England Patient Safety Response Standards, (2022) to provide resources and the training required for this to happen.
We will have governance arrangements in place to ensure patient safety learning responses are not led by NWAS staff who were involved in the patient safety event itself. Responsibility for patient safety learning responses from our locally agreed NWAS priorities sits with the Patient Safety Incident Response Team.
Patient Safety Learning Responses (PSLRs) sitting outside of our priorities will be led by a suitable senior leader within the relevant service line. Patient Safety Incident Learning Response Leads will have an appropriate level of seniority to influence within the trust, this may depend on the nature and complexity of the patient safety event and the learning response required.
The governance arrangements will ensure patient safety learning responses are not undertaken by staff working in isolation. Patient Safety Incident Response Team will support patient safety learning responses wherever possible and can provide advice on cross-system and cross-area working where this is required.
Our people affected by patient safety events will be afforded the necessary support and given time to participate in patient safety learning responses. All NWAS leaders will work within our just culture principles and utilise other teams to ensure our people are supported. NWAS service lines will ensure processes are adopted so leaders work within this framework to ensure psychological safety.
We will utilise both internal and (where necessary) external subject matter experts with relevant experience, knowledge, and skills.
NWAS has invested in one of the nationally mandated training providers from NHS England to ensure those with responsibility for responding and supporting patient safety events had adequate skills and knowledge to support those involved.
A training needs analysis has been developed and will be monitored on an ongoing basis, to ensure those with responsibility for, responding to and supporting patient safety events remains up-to date. This training will be delivered alongside an ambitious programme of safety skills training, including the Patient Safety Syllabus.
Our PSIRP sets out NWAS intends to respond to patient safety events over a period of 12-to-18-month period. The plan is not a permanent set of rules that cannot be changed. We will remain flexible and consider the specific circumstances in which each patient safety event occurred, and the needs of those affected as well as the plan. A copy of our PSIRP can be located on both our internal platform, the Greenroom, and our website.
Our PSIRP is a “live document” that will be appropriately amended and updated as we use it to respond to patient safety events. We will review the plan regularly, and at least annually to ensure our focus remains up to date, with ongoing improvement work, our patient safety profile is likely to change.This will also provide an opportunity to re-engage with stakeholders to discuss and agree any changes made in the previous 24 months.
Updated PSIRP and policy will be published on our website, replacing the previous versions.
A rigorous planning exercise will be undertaken every four years and more frequently if appropriate (as agreed with our lead Integrated Care Board) to ensure efforts continue to be balanced between learning and improvement.
This more in-depth review will include our response capacity, mapping services, a wide review of organisational data (patient safety incident reports, improvement plans, complaints, claims, staff survey results, inequalities data and any other relevant reporting data) and wider stakeholder engagement.
All our people (staff and volunteers) are responsible for recording and reporting potential or actual patient safety events on the trusts DCIQ system. The reporter will record the level of harm they believe to have been experienced by those affected. Each patient safety record will be reviewed and triaged by a corporate team and allocated to the relevant service line(s) for review, response, feedback to the reporter and closure.
The organisation has corporate oversight of all patient safety events and service lines have their own mechanisms in place to ensure patient safety events are responded to proportionately and in a timely manner. This will include consideration of Duty of Candour (Duty of Candour Procedure, found on the Green Room here ). Most events will require a local review and learning response (if necessary), undertaken by individual service lines. Those events where the opportunity to learning and improvement would be of greatest value, will be led by the trust Patient Safety Incident Learning Response Team.
Events and/or incidents highlighted that appear to meet requirements for reporting externally will be handled by the Patient Safety Incident Learning Response Team. There will be occasions where events require the efforts of cross-system working with relevant partners, the Integrated Care Board (ICB) will support a collaborative approach with these arrangements if required.
NWAS will have arrangements in place to meet the requirement to review patient safety events under PSIRF. Some of these will require a mandatory response, others will require review or referral to another body and/or team; these are set out in the PSIRF plan.
PSIRF itself sets no further national thresholds to determine what method of response should be utilised for learning and improvement. NWAS has developed a range of response mechanisms to balance the efforts between learning and exploring emerging issues alongside ongoing improvement work. During the work to create our plan, we considered our event insight and engagement with key stakeholders to identify our patient safety profile. We have used and will build on this intelligence for our local priorities and our toolkit for responding to patient safety events.
We have established a process for our response to events, that allows for a clear set of mechanisms allowing for oversight of our learning responses.
We will hold a weekly decision-making governance meeting to review events from escalation within service lines, and a decision is made on an appropriate level of response, this is to identify those events that appear to meet the need for further exploration due to the possibility of meeting the criteria for a full review. This group will have delegated responsibility for the consideration of events for PSII (Patient Safety Incident Investigation) or a patient safety learning response for oversight of outcomes. All recommendations made will focus on system-based approaches utilising the SEIPS (systems engineering initiative for patient safety) model, ensuring recommendations are valid and contribute to existing safety improvement plans or establishment of such, if they are required.
The Quality and Performance Committee will hold overall oversight of such processes, allowing for challenge where required, to ensure the Board of Directors can be assured the true intent of PSIRF is being implemented across our organisation to ensure we are meeting to the national response standards.
The Patient Safety Incident Response Team will assist in the coordination of these events identified to other providers directly, via each organisations reporting processes. Where required summary reporting can be utilised to share insights with other providers about their patient safety profile.
We will work with partner providers and relevant ICBs to establish and maintain robust procedures to facilitate flow of information and minimise delays to joint working on cross-system events. The patient safety team will act as a single access point for such working arrangements and hold supportive procedures to ensure this is effectively managed.
NWAS will refer to ICBs to assist with the coordination where a cross-system event is felt to be complex to be managed by a single provider, we anticipate the ICB will provide support and advice with identifying a suitable reviewer, should this circumstance arise.
Where a full PSII is indicated, this will be started as soon as practically possible following the identification and completed within three months. Locally – led PSIIs should not exceed six months.
Timeframe for completion will be agreed with those affected, as part of setting the terms of reference; this remains subject to them willing and able to be involved in that decision. A balance will be drawn between conducting a thorough review, the impact extended timescales can have on those involved and the risk of delaying findings may adversely affect safety.
In exceptional circumstances (i.e., when a partner organisation requests a pause, or processes of external bodies delay access to information) NWAS can consider whether to progress and determine whether new information would indicate the need for further review once this is received. The decision for this would be made by the Patient Safety Event Cases (PSEC) group.
There may be occasions where a longer timeframe is required for completion, in this case, all extended timeframes will be agreed between NWAS and those affected.
A Patient Safety Learning Response must be started as soon as practically possible following a patient safety event is identified. These learning responses should not exceed six months in duration.
NWAS acknowledges any form of patient safety learning response will allow the circumstances of an event or set of events to be understood, but this may only be the beginning. To reliably reduce risk, better safety actions are required.
We will have systems and processes in place to design, implement and monitor safety actions using an integrated approach of reducing risk and limit the potential for future harm. This process follows from any initial findings of any form of learning response which could result in aspects of trust’s working systems where change could reduce risk and harm. NWAS will generate safety actions in relation to each of these defined areas for improvement. Following this, we will have measures to monitor safety actions and set milestones for review.
Patient Safety Learning Responses should not describe recommendations, as this can lead to premature attempts to devise a solution. To achieve successful improvement, safety action development will be completed in collaborative way with a flexible approach and support from the Quality, Improvement, and Innovation Directorate.
NWAS will utilise processes for development of safety actions as outlined by NHS England; Safety Action Development Guide, (2022):
Safety actions must continue to be monitored within service lines governance arrangements to ensure any actions put in place remain impactful and sustainable.
Safety improvement plans bring together findings from various responses to patient safety events and issues. NWAS will have several safety improvement plans in place which are adapted to respond to outcomes of improvement efforts and other influences as national safety improvement programmes.
The NWAS PSIRP has outlined local priorities for focus or response under the PSIRF. These were developed due to the opportunity they offer for learning an improvement across areas where there is no existing plan or where improvement efforts have not been accompanied by reduction in risk or harm.
The trust will use the outcomes from existing patient safety reviews and any relevant learning response conducted under PSIRF to create related improvement plans to assist focus on our improvement work. NWAS service lines will work collaboratively with NWAS Corporate Teams and others to ensure there is an aligned approach to development of plans and resultant improvement efforts.
Where overarching systems issues are identified by patient safety learning responses outside of trust priorities, a safety improvement plan will be developed. These will be identified through the PSIRF governance processes. Monitoring of progress for safety improvement plans, will be overseen by Regional Improvement and Learning Forum on a scheduled basis.
Working under PSIRF, organisations are advised to design oversight systems to allow an organisation to demonstrate improvement rather than compliance with centrally mandated measures. NWAS follows the “mindset” principles to underpin the processes we have in place to allow us to implement PSIRF as set out in the framework and supporting guidance.
Alongside the Trust’s responsibilities, our lead ICBs, and our regulator the Care Quality Commission (CQC), will have specific responsibilities under PSIRF.
The Trust Board is responsible and accountable for effective patient safety incident management across NWAS. This includes supporting and participating in cross-system/ multi-agency responses, and/or independent patient safety incident investigations (PSIIs) where required.
To meet these requirements, NWAS has designated the Director of Corporate Affairs as the executive lead to support PSIRF. This enables us to:
The Director of Corporate Affairs will provide direct leadership, advice, support in complex/ high profile cases, and liaise with external bodies, as required, in collaboration with the Director of Quality, Innovation and Improvement and the Medical Director.
The Director of Corporate Affairs has the overarching responsibility for the quality of patient safety learning responses and PSIIs. The Director of Quality, Innovation and Improvement has the overarching responsibilities for safety learning and improvement. The Medical Director is overall accountable for patient safety for the Trust.
Each Executive Director are equipped with the training and professional development as described in the national patient safety incident response standards
NWAS recognises that there will be occasions when patients, services users and carers are dissatisfied with the aspects of care and services provided by the trust.
It is important to understand that there is a distinction between complaints and concerns as the use of the word complaint should not automatically mean that someone expressing a concern enters the complaints process.
The first point of contact with the trust, to raise a concern is via the PALS team.
Complaints are defined as expressions of dissatisfaction from a patient, their family or carer, a person acting as their representative or any person who is affected or likely to be affected by the action, omission or decision of the trust and requires a formal review.
NWAS is committed to dealing with any complaints that may arise quickly and as effectively as possible as set out in the Local Authority Social Services and National Health Service Complaints (England) Regulations 2009.
Complaints will be handled respectfully ensuring that all parties concerned feel involved in the process and assured that the issues raised have been comprehensively reviewed and the outcomes shared in an open and honest manner.
Complaints and concerns can be valuable aids in developing and maintaining standards of care and that lessons learnt from complaints can be used positively to improve services. Outcomes and recommendations from a complaint will be shared with service lines to ensure any necessary changes can be considered and implemented where appropriate.
If patients, relatives and or carers have a concern or complaint in relation to how a patient safety learning response has or is being handled, they should contact their nominated Patient Safety Incident Learning Response Lead or Engagement Lead in the first instance. Every effort will be made to address specific concerns.
This Patient Safety Incident Response Plan (PSIRP) sets out how North West Ambulance Service NHS Trust (NWAS) intends to respond to patient safety events over a 12 to 18 month period, however, the plan is not a permanent rule that cannot be changed. We will remain flexible and consider the specific circumstances in which patient safety issues and incidents occurred and the needs of those affected.
The NHS Patient Safety Strategy was published in July 2019 and describes the Patient Safety Incident Response Framework (PSIRF), a replacement of the NHS Serious Incident Framework. The Serious Incident Framework provided structure and guidance on how to identify, report, and investigate an incident resulting in severe harm, or death. PSIRF is best considered as a learning and improvement framework with the emphasis placed on systems and culture that support continuous improvement in patient safety through how NWAS responds to patient safety incidents.
The NHS Patient Safety Strategy, 2019 describes PSIRF as ‘a foundation for change’ and as such, it challenges us to think and respond differently when a patient safety incident occurs. One of the underpinning principles of PSIRF is to carry out fewer ‘investigations’ but make them better. Better means taking the time to conduct systems-based learning responses by people that have been trained to do them. This PSIRP and associated organisational policies and guidelines will describe how it all works. The NHS Patient Safety Strategy challenges us to think differently about learning and what it means for healthcare organisations.
Carrying out learning responses for the right reasons can and does identify meaningful learning. The removal of the serious incident process does not mean ‘do nothing’, it means respond in the right way depending on the type of incidents and associated factors.
A risk to the successful implementation of PSIRF at NWAS is continuing to ‘investigate’ and review incidents as we have done previously and simply give the process a new label, however, the challenge is to embed new language, and an approach to learning responses that forms part of the wider response to patient safety incidents whilst allowing time to learn thematically from other patient safety insights.
PSIRF recognises the need to ensure we have support structures for those involved in patient safety incidents (patients, families, and our people), part of which is the fostering of a psychologically safe culture demonstrated by all our leaders and supported by trust-wide strategies, and associated reporting systems.
NWAS has developed our understanding and insights over two to three years, including discussions and engagement through our internal governance processes, and with external stakeholders. This plan provides the headlines and description of how PSIRF will be applied at NWAS.
Our PSIRP should be read in conjunction with the Trust’s Patient Safety Incident Response Policy.
Our EOCs receive and triage 999 calls from members of the public as well as well as other emergency services. EOC staff provide advice and dispatch an ambulance to the scene as appropriate. The Clinical Hub (CHUB) is based within the EOC and assesses patients via telephone and provides the most appropriate care based on that assessment, known as hear and treat. This may be an ambulance (either emergency or urgent care), General Practitioner (GP) referral, referral to other services or self-care.
We deliver NHS 111 services for the North West region and are major contributors to the delivery of integrated urgent care. We signpost patients to the most appropriate care highlighted to them following triage and informed by the Directory of Services.
These can be solo responders or double crewed ambulances providing emergency care to the population of the North West.
Our PTS provide essential transport to non-emergency patients, in Cumbria, Lancashire, Merseyside, and Greater Manchester, who are unable to make their own way to and from hospital, outpatient clinics, or other treatment centres.
Our Hazardous Area Response Team (HART) and resilience teams are specially trained and equipped Paramedics who provide ambulance response to high-risk and complex emergency situations, including major incidents. They deliver our statutory responsibilities as a Category 1 responder under the Civil Contingencies Act (2004).
NWAA is an independent charitable organisation, whose strength lies in working collaboratively with strategic partners to deliver joined-up healthcare interventions, which achieve the best outcomes for the most unwell and critically injured patients. NWAA collaborates with NWAS, working together, we are able to deliver an integrated approach to pre-hospital care.
We have one of the largest and longest-established CFR schemes in England, with some 567 active CFRs operating across all areas of the North West, providing an effective service in their local communities. CFRs are volunteers who live and work in local communities, trained and activated by our EOCs to attend certain calls, such as chest pain or cardiac arrest, where response time can make the difference between life and death. CFRs provide care and support to the patient until the arrival of an emergency ambulance. All CFRs are equipped appropriately to respond to the emergency they are sent to, they have access to the required levels of personal protective equipment (PPE) for their skill set and we continually review this to ensure it aligns with both organisational and national requirements.
Our Patient Transport Volunteer Car Drivers play an invaluable role in transporting patients to and from hospital appointments including renal dialysis, oncology, and routine appointments. The 190 operational volunteers operate across the North West and transport patients in their own vehicles whilst offering a friendly face and listening ear, putting patients who are often anxious or concerned about their appointment at ease.
NWAS has a commitment to learning from patient safety events and we have continuously developed our understanding and insights into patient safety matters over a number of years.
PSIRF sets no rules or thresholds to determine what needs to be learned from to inform improvement apart from the national requirements listed on page 10. To fully implement PSIRF, NWAS has completed a holistic review of patient safety data insights to understand areas of learning to inform improvement.
NWAS has engaged with key stakeholders, both internal and external and undertaken a review of data from various sources to arrive at a patient safety profile. This process has also involved identification and specification of the methods used to maximise learning and improvement. This has led to the development of the NWAS Local Priorities as listed on page 12.
NWAS commenced planning for PSIRF following the release of the national documents from NHS England in August 2022. We have consulted extensively with several PSIRF early adopters to enable understanding of the practicalities of planning for and implementing PSIRF. The assistance received from early adopters has been invaluable.
PSIRF requires a different approach to the oversight of patent safety incidents. NWAS has engaged with the Ambulance Commissioning Team, historically part of NHS Blackpool CCG prior to the formation of Integrated Care Services (ICSs) as they are currently responsible for the oversight of our application of the Serious Incident Framework. NWAS has continued to engage with the Ambulance Commissioning Team and Lancashire and South Cumbria ICS to explore how PSIRF will affect the reporting and management for them.
Internally, various communication methods have been used to outline the significant differences between PSIRF and the Serious Incident Framework including engagement workshops held with key stakeholders, including those from the Trust’s service lines. During these engagement workshops, the existing processes that are in place to manage and review patient safety events have been discussed to understand how these can be improved and identify new ways of working under PSIRF.
A resource analysis exercise was undertaken to understand the current resource and capacity for responding to patient safety incidents.
The data sources and how they were used to define our patient safety profile is detailed below. Once the data has been collated, it was shared with internal and external stakeholders supported by a number of engagement workshops to collectively review the data and finalise our Local Priorities.
To define our patient safety profile, data was taken from a variety of sources including assurance reports and data held within our Trust’s Governance, Risk, and Compliance system, DatixWeb and Datix Cloud IQ (DCIQ). The Trust collated data over a three-year period and recognised the possibility of skew in the data arising from the COVID-19 pandemic.
We have also considered feedback and information provided by our stakeholders, and subject matter experts as part of the data collection process. Data and information (both qualitative and quantitative) have therefore been received from the following sources:
Where it has been possible, we have considered elements of the data regarding health inequalities. As part of our engagement workshops, we have also considered new and emergent risks relating to future operational changes and changes in demand that historical data may not reveal.
The themes from the data sources were considered and discussed leading to the identification of our Local Priorities for a Patient Safety Incident Investigation (PSII) under PSIRF.
NWAS acknowledges whilst the defined list of Local Priorities has been agreed, this list is not fixed forever.
Our commitment is, that where a new risk emerges or learning, and improvement can be gained from a PSII into a particular incident or theme, this will be commissioned.
The Trust has been continually developing its governance arrangements and associated processes to ensure it gains insight from all patient safety events, and how this can result in local, or corporate quality improvement activity. NWAS has and will continue, to draw on guidance and feedback from national and regional level NHS bodies, regulators, Integrated Care Boards (ICBs), partner providers, and other key stakeholders to identify and assist with defining associated learning and improvement work we undertake.
NWAS uses the Model for Improvement framework approach. This is led by the Quality, Innovation, and Improvement Directorate and gives our people the tools to ensure improvement is sustained.
We plan to focus our efforts moving forwards on the development of safety improvement plans across our most significant patient safety improvement types, either those within the national requirements, or those identified in our Local Priorities. NWAS will remain flexible and consider improvement planning as required where a risk or patient safety issue emerges from our own internal or external surveillance.
Recommendations from Patient Safety Incident Learning Responses, and PSIIs, must be translated into effective and sustained improvement action(s) with a focus on reducing risk. For this to occur, NWAS will apply knowledge of the science of patient safety and improvement to identify:
NWAS has several programmes and projects alongside patient safety improvement plans that are in progress. These relate to full programmes of work, as opposed to individual activities. They have been designed and prescribed to address known issues to patient safety.
This section details the programmes, project and current quality improvement plans, their area and who they are monitored by.
Given that the Trust has finite resources for patient safety incident learning responses, NWAS intends to use those resources to maximise learning and improvement outcomes. PSIRF allows organisations to do this, rather than repeatedly responding to patient safety incidents based on subjective thresholds and definitions of harm, from which new learning will be limited.
Some patient safety incidents, such as Never Events and deaths thought more likely than not due to problems in care will always require a Patient Safety Incident Investigation (PSII) to learn and improve. For other types of patient safety incidents which may affect a particular cohort of patients, a PSII will also be required. These have been determined nationally, NWAS fully endorses this approach as this will align with our aim to learn and improve within a just and restorative culture.
As well as PSIIs, some patient safety incident types require specific reporting and/or review processes to be followed. For clarity, all types of incidents that have been nationally defined as requiring a specific response will be reviewed according to the suggested methods and are detailed in the table below.
National guidance recommends 20 to 25 Patient Safety Incident Investigations per year. Attempting to do more than this will impede our ability to adopt a systems-based approach from thematic analysis and learning from excellence.
Incidents meeting the Never Events Criteria 2018.
Approach is the PSII, and the improvement is to create local organisational recommendations and actions.
Approach is the PSII, and the improvement is to create local organisational recommendations and actions.
Approach is the PSII, and the improvement is to create local organisational recommendations and actions.
Approach is to refer to the NHS England Regional Independent Investigation Team for consideration for an independent PSII. Locally led PSII may be required. The improvement is to Respond to recommendations from external referred agency/ organisation as required and feed actions into quality improvement work.
The approach is to refer to HSIB or SpHA for independent PSII. The improvement is to respond to recommendations from external referred agency/ organisation as required. Feed actions into quality improvement work.
The approach is to refer to Child Death Overview Panel (CDOP) review. Locally led PSII (or other response) may be required alongside the CDOP review. NWAS is to liaise with the CDOP in these circumstances. The improvement is to respond to recommendations from external referred agency/ organisation as required. Feed actions into quality improvement work.
The approach is to refer for Learning Disability Mortality Review (LeDeR). Locally led PSII (or other response) may be required alongside the LeDeR. NWAS is to liaise with this review. the improvement is to respond to recommendations from external referred agency/ organisation as required, and Feed actions into quality improvement work.
The NWAS named Safeguarding Lead will contribute towards domestic independent inquires, joint targeted area inspections, child safeguarding practice reviews, domestic homicide reviews and any other safeguarding reviews (and inquiries) as required to do so by the local safeguarding partnership (for children) and local safeguarding adult boards.
The improvement is to respond to recommendations from external referred agency/ organisation as required. Feed actions into quality improvement work.
The approach is to refer to Local Screening Quality Assurance Service for consideration of locally led learning response.
The improvement is to respond to recommendations from external referred agency/ organisation as required. Feed actions into quality improvement work.
The approach to any death in prison or police custody is that it will be referred (by the relevant organisation) to the Prison and Probation Ombudsman (PPO) or the Independent Office for Police Conduct (IOPC) to carry out the relevant investigations. NWAS will fully support these investigations where required to do so.
The improvement is to respond to recommendations from external referred agency/ organisation as required. Feed actions into quality improvement work.
The approach is Identified by the police usually in partnership with the Community Safety Partnership (CSP) with whom the overall responsibility lies for establishing a review of the case.
Where the CSP considers that the criteria for a domestic homicide review (DHR) are met, it uses local contacts and requests the establishment of a DHR panel. NWAS will contribute as required by the DHR panel.
The improvement is to respond to recommendations from external referred agency/ organisation as required. Feed actions into quality improvement work.
PSIRF allows organisations to explore patient safety incidents relevant to their context and the population served. Through analysis of our patient safety insights, based on the review of multiple data sources, and engagement workshops held, NWAS has determined that the Trust will focus on three Local Priorities for focus.
This number of Local Priorities have been selected due to the breadth and complexity of the services NWAS provides. National guidance recommends that 3 to 6 learning responses per priority are conducted per year. Attempting to do more than this will impede our ability to adopt a systems-based learning approach from thematic analysis and learning from excellence.
The Local priorities identified for a Patient Safety Incident Investigation (PSII) have been agreed by the Trust’s Executive Leadership Committee (ELC), Quality and Performance Committee, and the Board of Directors for the next 12 to 18 months.
The following events require a PSII approach and have the improvement of creating local organisational recommendations & actions that feed into the Safety Improvement Plan:
Any unexpected safety event that carries a level of risk and/or learning for patients/ families/ carers, healthcare staff or organisations that is so great (within or across the healthcare system), where the contributory factors are not widely understood and therefore warrants the use of extra resources to mount a comprehensive PSII response.
For any patient safety incident not meeting the PSII response, or any other incident, we will use appropriate and proportionate approaches as outlined within the PSIRF. For lesser harm incidents, NWAS propose to manage these at a local level with ongoing thematic analysis, with findings being reported via the PSIRF governance arrangements. This may lead to new or supplement existing improvement work.
Ladybridge Hall,
Chorley New Road,
Bolton,
BL1 5DD.
1.1.3 NHS Trusts are governed by statute, mainly the National Health Service Act 1977 (NHS Act 1977), the National Health Service and Community Care Act 1990 (NHS & CC Act 1990) as amended by the Health Authorities Act 1995, the Health Act 1999 and the Health and Social Care Act 2012. The statutory functions are conferred by this legislation.
1.1.4 As a statutory body, the Trust has specific powers to contract in its own name and to act as a corporate trustee. In the latter role it is accountable to the Charity Commission for those funds deemed to be charitable as well as to the Secretary of State for Health and Social Care.
1.1.5 The Membership and Procedure Regulations (1990) as amended requires the Trust to adopt Standing Orders for the regulation of its proceedings and business. The Trust must also adopt Standing Financial Instructions as an integral part of Standing Orders setting out the responsibilities of individuals.
1.1.6 These Standing Orders apply to the North West Ambulance Service NHS Trust and its statutory elements.
The Chair of the Trust is the final authority in the interpretation of Standing Orders (on the advice of the Chief Executive and Director of Corporate Affairs).
| Terminology | Definition |
| Accountable Officer | Is the officer responsible and accountable for funds entrusted to the Trust; and is responsible for ensuring the proper stewardship of public funds and assets. The Chief Executive, or their appointed replacement, is the Accountable Officer for this Trust |
| Board of Directors | The Board of Directors means the Chair; Non-Executive Directors and both voting and non-voting Executive Directors. |
| Chair of the Board of Directors | Is the person appointed by the Secretary of State for Health and Social Care to lead the Board and to ensure that it successfully discharges its overall responsibility for the Trust as a whole. The expression “the Chair of the Trust” shall, if the Chair is absent from the meeting or otherwise unavailable, be deemed to include the Vice-Chair of the Trust, or other Non-Executive Director. |
| Chief Executive | The Accountable Chief Officer of the Trust |
| Committee | A committee appointed by the Board of Directors |
| Committee Members | Formally appointed by the Board of Directors to sit on, or to chair specific committees |
| Directors | Are the Non-Executive Directors and Executive Directors (including non-voting Directors) |
| Director of Finance | The Chief Financial Officer of the Trust |
| The Trust | North West Ambulance Service NHS Trust |
| Funds held on Trust | Are those funds which the Trust holds at its date of incorporation, receives on distribution by statutory instrument, or chooses subsequently to accept under powers derived under Part 11 (eleven) of the NHS Act 2006. Such funds may or may not be charitable. |
| Motion | A formal proposition to be discussed and voted on during the course of a Board of Directors or Committee meeting |
| Nominated Officer | An Officer charged with the responsibility for discharging specific tasks within Standing Orders and Standing Financial Instructions |
| Officer | An employee of the Trust or any other person holding a paid appointment or office with the Trust |
| Secretary | A person appointed to act independently of the Board to provide advice on corporate governance issues to the Board and the Chair and monitor the Trust’s compliance with the Law, Standing Orders and Department of Health guidance |
| Vice Chair | The Non-Executive Director appointed by the Trust to take on the chair’s duties is the Chair is absent for any reason |
| All reference to the masculine gender shall be read as equally applicable to the feminine gender and vice-versa. | |
1.4.1 In addition to the statutory requirements the Secretary of State through the Department of Health and Social Care issues further directions and guidance. These are normally issued under cover of a circular or letter. The majority of these can be found on the department of health website.
1.4.2 The Code of Accountability for NHS Boards requires that, inter-alia, Boards draw up a schedule of decisions reserved to the Board known as the ‘Reservation of Powers to the Board’ and ensure that management arrangements are in place to enable responsibility to be clearly delegated to senior executives through a Scheme of Delegation. The Code also requires the establishment of Audit and Remuneration Committees with formally agreed terms of reference. The Code of Conduct for NHS Boards makes various requirements concerning possible conflicts of interest of members of the Board.
1.4.3 The Code of Practice on Openness in the NHS or the Freedom of Information Act 2000 and sets out the requirements for public access to information on the NHS.
1.5.1 The Trust has powers to delegate and make arrangements for delegation. These Standing Orders set out the detail of these arrangements. Under the Standing Order relating to the Arrangements for the Exercise of Functions by Delegation (SO5), the Board is given powers to ‘make arrangements for the exercise, on behalf of the Trust, of any of their functions by a Committee, Sub Committee or Joint Committee appointed by virtue of SO4 or by an Officer of the Trust, in each case subject to such restrictions and conditions as the Trust sees fit or as the Secretary of State for Health and Social Care may direct’. Delegated powers are included within these Standing Orders and (Reservation of Powers to the Board and Scheme of Delegation). The Standing Financial Instructions is a separate document. These documents have effect as if incorporated into these Standing Orders.
Trust Boards are now encouraged to move away from silo governance and develop integrated governance that will lead to good governance and ensure that decision-making is informed by intelligent information. Integrated governance better enables the Board to take a holistic view of the organisation and its capacity to meet its legal and statutory requirements and clinical, quality and financial objectives.
2.1.1 In accordance with the Establishment Order 2006 No 1662 and Membership and Procedure Regulations 1990 (as amended) the voting membership of the Board of Directors shall comprise the Chair and five Non-Executive Directors, together with up to five Executive Directors. At least half of the membership of the Trust Board, excluding the Chair, shall be independent Non-Executive Directors.
In addition to the Chair, the Non-Executive Directors shall normally include:
The Voting Executive Directors shall include:
The Board may appoint additional Executive Directors, to be non-voting members of the Trust Board, these currently include:
2.2.1 The Chair and Non-Executive Directors of the Trust are appointed by NHSE, on behalf of the Secretary of State for Health and Social Care.
2.2.2 Associate Non-Executive Directors are appointed by the Trust.
2.2.3 The Chief Executive is appointed by the Chair and the Non-Executive Directors.
2.2.4 Other Executive Directors/Directors shall be appointed by a committee comprising the Chair and the Non-Executive Directors, under recommendation from the Chief Executive.
2.2.5 Where more than one person is appointed jointly to an Executive Director post in the Trust, those persons shall become appointed as an Executive Director, jointly. Where the post has voting rights attached, the joint appointees will have the power of one vote; and shall count as one person.
2.3.1 The regulations governing the period of tenure of office of the Chair and Non-Executive Directors and the termination or suspension of office of the Chair and Non-Executive Directors are contained in the Membership and Procedure Regulations and as directed by NHSE, under its delegated authority from Secretary of State for Health and Social Care.
2.3.2 In line with NHS England’s Code of Governance for NHS Provider Trusts, Chairs and Non-Executive Directors should not remain in post beyond nine years from the date of their first appointment and any decision to extend a term beyond nine years should be subject to rigorous review and consideration of progressive refreshing of the Board should be taken into account. In exceptional circumstances, terms may be extended for a limited time beyond nine years however should be subject to annual re-appointment by NHS England. Serving more than nine years could be relevant to the determination of a non-executive’s independence.
2.4.1 To enable the proceedings of the Trust to be conducted in the absence of the Chair, the Board of Directors may elect one of the Non-Executive Directors to be Vice-Chair, for a period that does not exceed the remainder of their appointed term as a Non-Executive Director of the Trust.
2.4.2 Any Non-Executive Director so elected may at any time resign from the office of Vice-Chair by giving notice in writing to the Chair. The appointment as Vice-Chair will end with the termination for any reason of that Non-Executive Director’s period of office as a director. On such resignation or termination the Board of Directors may then appoint another Non-Executive Director as Vice-Chair, in accordance with the provision of this Standing Order.
2.4.3 When the Chair is unable to perform their duties due to illness or absence for any reason, his duties will be undertaken by the Vice-Chair who shall act as Chair until a new Chair is appointed or the existing Chair resumes their duties.
2.4.4 In order to appoint the Vice-Chair, nominations will be invited by the Chair. Where there is more than one nomination, a vote will be conducted and the results announced at the subsequent meeting of the Board. In the event of there being only one nomination and this being acceptable to the Directors present, the Board will be requested to confirm that person as Vice-Chair at the meeting in which the nomination is made.
2.5.1 The Board will function as a corporate decision-making body, Officer and Non-Officer members will be full and equal members. Their role as members of the Board of Directors will be to consider the key strategic and managerial issues facing the Trust in carrying out its statutory and other functions.
Executive Members shall exercise their authority within the terms of these Standing Orders, Standing Financial Instructions and the Scheme of Delegation.
The Chief Executive shall be responsible for the overall performance of the executive functions of the Trust. He/she is the Accountable Officer for the Trust and shall be responsible for ensuring the discharge of obligations under Financial Directions and in line with the requirements of the Accountable Officer Memorandum for Trust Chief Executives.
The Director of Finance shall be responsible for the provision of financial advice to the Trust and to its members and for the supervision of financial control and accounting systems. He/she shall be responsible along with the Chief Executive for ensuring the discharge of obligations under relevant Financial Directions.
The Non-Executive Members shall not be granted nor shall they seek to exercise any individual executive powers on behalf of the Trust. They may however, exercise collective authority when acting as members of or when chairing a committee of the Trust which has delegated powers.
The Chair shall be responsible for the operation of the Board and chair all Board meetings when present. The Chair must comply with the terms of appointment and with these Standing Orders.
The Chair shall work closely with the Chief Executive and ensure that key and appropriate issues are discussed by the Board in a timely manner, together with all necessary information and advice being made available to the Board to inform the debate and ultimate resolutions.
The Senior Independent Director shall be available to hear any issues or concerns that individuals feel unable to raise with the Chair or any Executive Director.
2.5.2 In line with NHS England’s Code of Governance for NHS Provider Trusts, where directors have concerns about the operation of the Board or the management of the trust that cannot be resolved, these should be recorded in board minutes. In the case of the resignation of a Non-Executive Director, any such concerns should be provided in a written statement to the Chair for circulation to the Board.
2.6.1 All business shall be conducted in the name of the Trust.
2.6.2 All funds received in trust shall be in the name of the Trust as corporate trustee. In relation to funds held on trust, powers exercised by the Trust as corporate trustee shall be exercised separately and distinctly from those powers exercised as a Trust.
2.6.3 The powers of the Trust established under statute shall be exercised by the Board meeting in public session except as otherwise provided in SO3.
2.7.1 The Board has resolved that certain powers and decisions may only be exercised or made by the Board in formal session. These powers and decisions are set out in the Reservation of Powers to the Board and are incorporated into the Standing Orders. Those powers which it has delegated to individuals and other bodies are contained in the Scheme of Delegation.
3.1.1 All ordinary meetings of the Board of Directors shall be held in public and shall be conducted in accordance with relevant legislation, including the Public Bodies (Admission to Meetings) Act 1960, as amended and guidance issued by the Secretary for State for Health. Members of the public and representatives of the press shall be afforded facilities to attend.
3.1.2 Ordinary meetings of the Board of Directors shall be held at regular intervals at such times and places as the Board of Directors may from time to time determine. A minimum of six meetings shall be held each year.
3.1.3 The public and representatives of the press shall be afforded facilities to attend all formal meetings of the Board but shall be required to withdraw upon the Board resolving as follows:
‘That representatives of the press and other members of the public be excluded from the remainder of this meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest’
as required under s.1(2) of the Public Bodies (Admission to Meetings) Act 1960.
3.1.4 The Chair (or person presiding at the meeting) shall give such directions as he thinks fit in regard to the arrangements for meetings and accommodation of the public and representatives of the press such as to ensure that the Board’s business shall be conducted without interruption and disruption and, without prejudice to the power to exclude on the grounds of the confidential nature of the business to be transacted, the public will be required to withdraw upon the Board resolving as follows:
‘That, in the interests of public order, the meeting adjourn for [the period specified] to enable the Board to complete business without the presence of the public’
as required under s.1(8) of the Public Bodies (Admission to Meetings) Act 1960.
3.1.5 The Board of Directors or any employee or representative of the Trust in attendance at a private meeting or private part of a meeting, shall not reveal or disclose the contents of papers, discussions or minutes of the items taken in private, outside of the Board of Director meetings without express permission of the Board of Directors.
3.1.6 Nothing in these Standing Orders shall require the Board to allow members of the public or representatives of the press to record proceedings in any manner whatsoever, other than in writing, or to make any oral report of proceedings as they take place, without the prior agreement of the Board.
3.2.1 Regular meeting of the Trust
Agendas will be sent to members at least five days before the meeting. Supporting papers, whenever possible, shall accompany the agenda and will in any event be despatched no later than three clear days before the meeting, except in an emergency.
3.2.2 Exceptional meetings of the Trust
A notice of the meeting, specifying the business proposed to be transacted at it, and signed by the Chair or by an Officer of the trust authorised by the Chair to sign on their behalf, shall be delivered to every Director, so as to be available to them at least three clear days before the meeting.
3.2.3 Meetings called by Directors
In the case of a meeting called by Directors in the event that the Chair has not called the meeting, the notice shall be signed by those Directors and no business shall be transacted at the meeting other than that specified in the notice.
3.2.4 Public notice
Before each meeting of the Board, a public notice of the time and place of the meeting, and the public part of the agenda, shall be displayed at the Trust’s office at least three clear days before the meeting, as required under s.1(4)(a) of the Public Bodies (Admission to Meetings) Act 1960.
3.3.1 The Trust may determine that certain matters shall appear on every agenda for a meeting of the Trust and shall be addressed prior to any other business being conducted.
3.3.2 A Director may request that a matter is included on an agenda. This request should be made in writing to the Chair and Director of Corporate Affairs at least seven clear days before the meeting. The request should state whether the item of business is proposed to be transacted in the presence of the public and should include appropriate supporting information. Requests made less than seven days before a meeting may be included on the agenda at the discretion of the Chair.
3.3.3 Where a petition has been received by the Trust, the Chair shall include the petition as an item for the agenda of the next Board meeting.
The Trust will publicise and hold an annual public meeting in accordance with the NHS Trusts (Public Meetings) Regulations 1991. The meeting shall take place no later than 30 September each year. The Annual Report and Annual Accounts of the preceding year shall be presented at that meeting.
3.5.1 The Chair shall preside at any meeting of the Trust Board, if present. In their absence, the Vice Chair shall preside.
3.5.2 If the Chair and Vice-Chair are absent, the directors present, who are eligible to vote shall choose a Non-Executive Director who shall preside. An Executive Director may not take the chair.
3.5.3 The decision of the Chair of the meeting on questions of order, relevancy and regularity (including procedure on handling motions) and the Chair’s interpretation of the Standing Orders shall be final. In this interpretation the Chair shall be advised by the Director of Corporate Affairs and in the case of Standing Financial Instructions the Chair shall be advised by the Director of Finance.
3.6.1 It is not a requirement for decisions to be subject to a vote. The necessity of a vote shall be indicated by the agreement of at least one third of those attending and eligible to vote. The Chair shall be responsible for deciding whether a vote is required and what form this will take.
3.6.2 Where it is necessary to take a vote to determine an issue, the decision shall be determined by a majority of the votes of the directors present and eligible to vote. If the result of the vote is equal, the Chair of the meeting shall have a second or casting vote.
3.6.3 All questions put to the vote shall, at the discretion of the Chair of the meeting, be determined by oral expression or by a show of hands. A paper ballot may be held, if a majority of the directors present and eligible to vote, so request. Unless specifically agreed beforehand, the voting record of each individual director will not be made public, or recorded
3.6.4 The voting record, other than by paper ballot, of any question will be recorded to show how each director present voted or did not vote, if at least one-third of the directors present and eligible to vote so request.
3.6.7 An officer who has been appointed formally by the Trust to act up for an Executive Director during a period of incapacity, or temporarily to fill an Executive Director vacancy, shall be entitled to exercise the voting rights of that Executive Director. An officer attending the Board of Directors to represent an Executive Director during a period of incapacity or temporary absence, but without formal acting up status, may not exercise the voting rights of that Executive Director. An officer’s status when attending a meeting shall be recorded in the minutes.
3.6.9 Where necessary, a director may be counted as present when available constantly for discussions through an audio or video link and may take part in voting on an open basis.
3.7.1 No business shall be transacted at a meeting of the Board unless at least six of the Directors who are eligible to vote (including at least three Executive and three Non-Executive Directors with voting powers) are present.
3.7.2 An officer in attendance for an Executive Director but without formal acting up status may not count towards the quorum.
3.7.3 A director will not count towards the quorum on a matter where he is ruled to be ineligible to participate in the discussion, or vote, due to the declaration of a conflict of interest. If a quorum is not available for the passing of a resolution on any matter, that matter may be discussed further at the meeting, but no resolution can be made. That position shall be recorded in the minutes of the meeting.
3.8.1 The names of the directors and others invited by the Chair present at the meeting, shall be recorded in the minutes.
3.8.2 If a director is not present for the entirety of the meeting, the minutes shall record the items that were considered whilst they were present.
3.9.1 The minutes of the proceedings of a meeting shall be drawn up, entered in a record kept for that purpose and submitted for agreement at the next meeting.
3.9.2 There should be no discussion on the minutes, other than as regards their accuracy, unless the Chair considers discussion appropriate.
3.9.3 Any amendment to the minutes as to their accuracy shall be agreed and recorded at the next meeting and the amended minutes shall be regarded as the formal record of the meeting.
3.10.1 Subject to the provision of Standing Order 3.11 and 3.13 a director of the Trust desiring to move a motion shall give notice of this in writing, to the Chair, at least seven working days before the meeting. The Chair shall insert all such notices that are properly made in the agenda for the meeting. This Standing Order shall not prevent any motion being withdrawn or moved without notice on any business mentioned on the agenda for the meeting.
3.11.1 When a motion is under debate, no motion may be moved other than:
3.11.2 The proposer may withdraw a motion or amendment once moved and seconded with the concurrence of the seconder and the consent of the Trust Board.
3.12.1 The mover of a motion shall have a right of reply at the close of any discussion on the motion or any amendment to it.
3.13.1 Notice of a motion to rescind any decision of the Board of Directors (or general substance of any decision) which has been passed within the preceding six calendar months, shall bear the signature of the director who gives it and also the signature of four other directors who are eligible to vote.
3.13.2 When the Board of Directors has debated any such motion, it shall not be permissible for any director, other than the Chair to propose a motion to the same effect within a further period of six calendar months.
3.14.1 Except where this would contravene any statutory provision or any direction made by the Secretary of State for Health and Social Care, any one or more of the Standing Orders may be suspended at any meeting, provided that at least two-thirds of the directors of the Trust are present and the majority of those present, vote in favour of suspension.
3.15.1 These Standing Orders shall be amended only if:
4.1.1 Subject to such directions as may be given by the Secretary of State for Health and Social Care, the Board of Directors may appoint committees of the Trust.
4.2.1 The Standing Orders of the Trust, as far as they are applicable, shall apply with appropriate alteration to meetings of any Committees established by the Trust. In which case the term ‘Chair’ is to be read as a reference to the Chair of other Committees as the context permits and the term ‘member’ is to be read as a reference to a member of other Committees also as the context permits. There is no requirement to hold meetings of Committees established by the Trust in public.
4.3.1 Each such committee shall have such terms of reference and powers and be subject to such conditions (as to reporting back to the Board), as the Board shall decide and shall be in accordance with any legislation and regulation or direction issued by the Secretary of State for Health and Social Care. Such terms of reference shall have effect as if incorporated into the Standing Orders.
4.3.2 Approved Terms of Reference for all Board Committees shall be held by the Director of Corporate Affairs.
4.4.1 The Board of Directors shall authorise any delegation of powers to be exercised by its formally constituted Committees. The Board of Directors shall approve the terms of reference of these committees and any specific powers.
4.5.1 The Board shall approve the appointments to each of the Committees which it has formally constituted. Where the Board determines and regulations permit that persons, who are not Directors, shall be appointed to a Committee, the terms of such appointment shall be determined by the Board.
4.6.1 Where the Trust is required to appoint persons to a Committee and/or to undertake statutory functions as required by the Secretary of State for Health and Social Care, and where such appointments are to operate independently of the Trust such appointment shall be made in accordance with the regulations laid down by the Secretary of State for Health and Social Care.
4.7.1 Minutes, or a representative summary of the issues considered and decisions taken, of any Committee appointed under this Standing Order are to be formally recorded. The Chair of such Committees are to provide a representative summary of the issues considered and any decisions taken to the next Board of Directors meeting.
The mandated committees to be established by the Board are:
The Board of Directors shall appoint a committee to undertake the role of an audit committee. This role shall include providing the Board of Directors with an independent and objective review of the financial systems and of general control systems that ensure the Trust achieves its objectives, the reliability of the financial information used by the Trust and of compliance with laws, guidance and regulations and codes of conduct governing the NHS. The Committee will comprise of a minimum of three Non-Executive Directors of which one must have significant, recent and relevant financial experience. This Committee will pay due regard to good practice guidance, including, in particular the NHS Audit Committee Handbook.
The Terms of Reference of the Audit Committee shall be approved by the Board of Directors and will be reviewed on a periodic basis.
The Board of Directors shall nominate its Audit Committee to act as its Audit Panel in line with schedule 4, paragraph 1 of the Local Audit and Accountability Act 2014.
The Audit Panel’s functions are to advise the Board of Directors on the selection and appointment of the External Auditor. This includes the following:
In line with the requirements of the 1990 Membership and Procedure Regulations, Regulations 17-18, a Remuneration Committee will be appointed and constituted to advise the Board about appropriate remuneration and terms of service for the Chief Executive and other Very Senior Managers including:
In line with its role as a corporate trustee for any funds held in trust, either as charitable or non-charitable funds, the Board will establish a Charitable Funds Committee to administer those funds in accordance with any statutory or other legal requirements or best practice required by the Charities Commission.
The Board of Directors shall appoint such additional non-mandatory committees as it considers necessary to support the business and inform the decisions of the Trust Board (Regulations 15-16, Membership and Procedure Regulations).
These are subject to change at the discretion of the Board of Directors. All new or amended non-mandatory committees will have the same standing and will be subject to the same standing orders.
5.1.1 Subject to Reservation of Powers to the Board, the Scheme of Delegation and such directions as may be given by the Secretary of State for Health and Social Care, the Board of Directors may delegate any of its functions to a committee appointed by virtue of SO4, or to a director or an officer of the Trust. In each case, these arrangements shall be subject to such restrictions and conditions as the Board thinks fit.
5.2.1 The powers which the Board of Directors has retained to itself within these Standing Orders may in emergency be exercised by the Chief Executive and the Chair acting jointly and after having consulted with at least two Non-Executive Directors and two Executive Directors. The exercise of such powers by the Chief Executive and the Chair shall be reported to the next formal meeting of the Board of Directors for ratification.
5.2.2 There may be instances where it is deemed critical for the Board of Directors to make a decision outside the time frames of a formal meeting. Such decisions should be agreed electronically (via email circulation) and the formal decision reported to the next formal meeting of the Board of Directors for formal ratification. A minimum quorum must be achieved for decisions reached outside formal meetings, wherever possible, the full Board of Director membership must reach any decision being made outside the meeting. The list of members involved must be reported to the next Board of Directors meeting alongside the formal ratification of the decision.
5.3.1 The Board of Directors shall agree from time to time to the delegation of specific powers to be exercised by committees, which it has formally constituted. The Board of Directors shall approve the constitution and terms of reference of these committees and their specific powers.
5.4.1 Those functions of the Trust, which have not been retained as reserved by the Board of Directors or delegated to a committee of the Trust Board, shall be exercised on behalf of the Board of Directors by the Chief Executive. The Chief Executive shall determine which functions he will perform personally and shall nominate officers to undertake the remaining functions for which he will still retain accountability to the Trust Board.
5.5.1 The Board of Directors shall adopt a Schedule of Decisions Reserved for the Board of Directors setting out the matters for which approval is required by the Trust Board.
5.5.2 The Board of Directors shall review such Schedule at such times as it considers appropriate; and shall update after each review.
5.5.3 The Schedule of Decisions Reserved for the Board of Directors shall take precedence over any terms of reference or description of functions of any committee established by the Trust Board. The powers and functions of any committee shall be subject to and qualified by the reserved matters contained in that Schedule.
5.6.1 The Board of Directors shall adopt a Scheme of Delegated Authorities setting out details of the directors and officers of the Trust to whom responsibility has been delegated for deciding particular matters; and in a director’s or officer’s absence, the director or officer who may act for them.
5.6.2 The direct accountability, to the Board of Directors, of the Director of Finance and other Executive Directors to provide information and advise the Board of Directors in accordance with any statutory requirements shall not be impaired, in any way, by the delegations set out in the Scheme of Delegated Authorities
If for any reason these Standing Orders are not complied with, full details of the non-compliance and any justification for non-compliance and the circumstances around non-compliance, shall be reported to the next formal meeting of the Board for action or ratification by the Director of Corporate Affairs. All members of the Board and all staff have a duty to disclose any non-compliance with these Standing Orders to the Chief Executive as soon as possible.
6.1.1 In addition to the statutory requirements relating to pecuniary interests, the Trust’s Standards of Business Conduct Policy requires Board members to declare interests annually, or as and when they arise, which are relevant and material to the NHS Board of which they are a member. All existing Board members should declare such interests. Any Board members appointed subsequently should do so on appointment.
6.1.2 Interests which should be regarded as relevant and material are:
6.1.3 If Directors have any doubt about the relevance of an interest, this should be discussed with the Director of Corporate Affairs.
6.1.4 At the time that Directors’ interests are declared they should be recorded in the Board minutes and the Register of Interests. Any changes in interests should be declared at the next Board meeting following the change occurring and will be recorded in the minutes of that meeting.
6.1.5 During the course of a Board meeting, if a conflict of interest is established, the Director(s) concerned should declare such likely conflict of interest and withdraw from the meeting unless requested to remain by the Board members present. The Director should play no part in the relevant discussion or decision.
6.2.1 The Chief Executive will ensure that a Register of Interests is established to record formally, declarations of interest of the Board. In particular the register will include details of all Directorships and other relevant and material interests which have been declared by both Executive and Non-Executive Directors, as defined in SO 6.1.2.
6.2.2 The Register of Interests shall be published on the website and shall be reviewed at least on an annual basis.
6.3.1 Subject to the following provisions of this Standing Order, which is taken from the Membership Procedure Regulations 1990 (as amended), if the Chair or a Director has any pecuniary interest, direct or indirect, in any contract, proposed contract or any other matter and is present at a meeting of the Board at which the contract or other matter is the subject of consideration, he shall at the meeting and as soon as practicable after its commencement, disclose the fact and shall not take part in the consideration or discussion of the contract or other matter or vote on any question with respect to it.
6.3.2 The Board may exclude the Chair or a member of the Board from a meeting of the Board while any contract, proposed contract or other matter in which that person has a pecuniary interest is under consideration.
6.3.3 Any remuneration, compensation or allowances payable to the Chair or a Director by virtue of the NHS (Consolidation) Act 2006 Schedule 3 Part 1 Paragraph 10, NHS Act 1997 Schedule 5A Paragraph 11(4) or the 1999 Act Schedule 1 (pay and allowances) shall not be treated as pecuniary interest for the purpose of this regulation.
6.3.4 Subject to SO 6.3.3 and any conditions imposed by the Secretary of State for Health and Social Care, the Chair or a Director shall be treated for the purpose of this regulation as having indirectly a pecuniary interest in a contract, proposed contract or other matter if:
6.3.5 For the purpose of clarity, the following definition of terms is to be used in interpreting this Standing Order:
6.3.6 The Chair or a Director shall not be treated as having a pecuniary interest in any contract, proposed contract or other matter by reason only:
The Secretary of State for Health and Social Care may, subject to such conditions as they may think fit to impose, remove any disability imposed by this Standing Order in any case in which it appears to them in the interests of the National Health Service that the disability shall be removed.
This regulation applies to a Committee of the Trust as it applies to the Board and applies to any member of any such Committee (whether or not they are also a Director of the Trust) as it applies to a Director of the Trust.
7.1.1 All staff must comply with the national guidance contained in HSG(93)5 ‘Standards of Business Conduct for NHS Staff’. The following provisions should be read in conjunction with that guidance and staff should also refer to the Trust’s Standards of Business Conduct; Policy on Managing Conflicts of Interest, Gifts & Hospitality and Sponsorship.
7.1.2 It is the responsibility of all Trust staff to ensure that they are not placed in a position which risks, or appears to risk, conflict between their private interests and their official duties.
7.1.3 It is an offence under the Bribery Act 2010 for an employee of the Trust to accept corruptly any inducement or reward for doing, or refraining from doing, anything in their official capacity, or corruptly showing favour or disfavour in the handling of contracts.
7.1.4 It is the responsibility of the Trust to ensure that its Officers are aware that breach of the provision of the Act renders them liable to prosecution and may also lead to the termination of their contracts of employment and superannuation rights within the NHS.
7.2.1 If it comes to the knowledge of a Director or an Officer of the Trust that a contract in which he has any pecuniary interest not being a contract to which he is himself a party, has been, or is proposed to be, entered into by the Trust he shall, at once, give notice in writing to the Chief Executive or Director of Corporate Affairs of the fact that he is interested therein. In the case of married persons or persons living together as partners, the interest of one partner shall, if known to the other, be deemed to be also the interest of that partner.
7.2.2 An Officer must also declare to the Chief Executive any other employment or business or other relationship of their partner, or of a co-habiting spouse, that conflicts, or might reasonably be predicted could conflict with the interests of the Trust.
7.2.3 The Trust will require interests, employment or relationships so declared to be entered in a register of interests of staff.
7.3.1 Canvassing of Directors of the Trust or members of any Committee of the Trust directly or indirectly, for any appointment under the Trust shall disqualify the candidate for such appointment. The contents of this paragraph of the Standing Orders shall be included in application forms or otherwise brought to the attention of candidates.
7.3.2 A Director of the Trust shall not solicit for any person, any appointment under the Trust or recommend any person for such an appointment. But this paragraph of Standing Orders shall not preclude a Director from giving written testimonial of a candidate’s ability, experience or character for submission to the Trust.
7.3.3 Unsolicited informal discussions outside appointment panels or Committees should be declared to the panel or Committee.
7.4.1 Candidates for any staff appointment shall when making an application, disclose in writing whether they are related to any Director or the holder of any office under the Trust. Failure to disclose such a relationship shall disqualify a candidate and, if appointed, render them liable to dismissal.
7.4.2 The Chair and every Director or Officer of the Trust shall disclose to the Board any relationship with a candidate of whose candidature that Director or Officer is aware. It shall be the duty of the Chief Executive to report to the Board any such disclosure made.
7.4.3 On appointment, Directors (and prior to acceptance of an appointment in the case of Executive Directors) should disclose to the Trust whether they are related to any other Director or holder of any office under the Trust.
7.4.4 Where the relationship of an Officer or another Director to a Director of the Trust is disclosed, the Standing Order headed ‘Exclusion of Chair and Members in Proceedings on Account of Pecuniary Interest ’ (SO 6.3) shall apply.
The common seal of the Trust shall be kept by the Director of Corporate Affairs in a secure place.
8.2.1 The Seal of the Trust shall only be attached to documents where the sealing has first been approved by the Trust Board, or the Chief Executive and the Director of Finance, or their designated acting replacement in accordance with the Scheme of Delegated Authorities
8.2.2 The seal shall be affixed in the presence of the signatories.
The Director of Corporate Affairs shall keep a register of sealings. An entry of every sealing shall be made and a report of all sealings shall be made to the Board at least bi-annually.
9.1 The Trust will from time to time, establish partnership arrangements (MoUs) with external organisations or groups (NHS or non NHS) with the aim of achieving identified benefits for the parties involved in the partnership.
9.2 For governance purposes, it is imperative that such partnership arrangements are subject to formal approval by the Trust Management Committee prior to any commitment to join the partnership.
9.3 The anticipated outcomes and duration of partnership arrangements will be measured and monitored by the relevant lead Officer. The Director of Corporate Affairs will maintain a register of partnership arrangements which will be presented to the Board for scrutiny on a 6 monthly basis.
9.4 For the avoidance of doubt, the definition of a Partnership is as follows:
‘A relationship established between the Trust and an external organisation for the furtherance or development of the Trust’s activities, which aim to deliver identified benefits to the satisfaction of all Partners in the relationship. Such relationships would be in addition to the purchaser/provider or client/customer relationships which arise through the Trust’s normal business activities.’
1.1 Standing Order 1.6 requires that the Trust must adopt a Reservation of Powers and Scheme of Delegation which define the powers retained by the Board. Those powers so determined are detailed below.
2.1 The Board may determine any matter, for which it has delegated or statutory authority, it wishes in full session within its statutory powers.
3.1.1 Approval of Standing Orders, a schedule of matters reserved to the Board and Standing Financial Instructions for the regulation of its proceedings and business.
3.1.2 Suspension of Standing Orders.
3.1.3 Approve variations or amendments to the Standing Orders, schedule of matters reserved to the Board and Standing Financial Instructions.
3.1.4 Ratify any urgent decisions taken by the Chair and Chief Executive in public session in accordance with SO5.2.
3.1.5 Ratify any decisions taken by the Board of Directors outside the timeframes of a normal meeting, in accordance with SO5.2.
3.1.6 Approval of a scheme of delegation of powers from the Board to committees and officers.
3.1.7 Require and receive the declaration of Board members’ interests that may conflict with those of the Trust and determining the extent to which that member may remain involved with the matter under consideration.
3.1.8 Require and receive the declaration of officers’ interests that may conflict with those of the Trust.
3.1.9 Approve arrangements for dealing and responding to complaints.
3.1.10 Receive reports from committees, including those that the Trust is required by the Secretary of State for Health and Social Care or other regulation to establish, and take appropriate action.
3.1.11 Confirm the recommendations of the Trust’s committees where the committees do not have executive powers.
3.1.12 Approve arrangements relating to the discharge of the Trust’s responsibilities as a corporate trustee for funds held on trust.
3.1.13 Establish terms of reference and reporting arrangements for all committees and sub-committees that are established by the Board.
3.1.14 Receive reports on instances of use of the seal.
3.1.15 Ratify, or otherwise, instances of failure to comply with Standing Orders or Standing Financial Instructions brought to the Chief Executive’s attention in accordance with SO5.7.
3.2.1 Approve and adopt the organisational structures, processes and procedures to facilitate the discharge of business by the Trust; and modifications thereto.
Require, from directors and officers, the declaration of any interests which might conflict with those of the Trust; and consider the potential impact of the declared interests.
3.2.2 Agree and oversee the approach to disciplining directors who are in breach of statutory requirements of the Trust’s Standing Orders.
3.2.3 Approve the disciplinary procedure for officers of the Trust.
3.3.1 Define the strategic aims and objectives of the Trust.
3.3.2 Approve all Trust strategies
3.3.3 Approve proposals for ensuring quality and developing clinical governance in services provided by the Trust, having regard to any guidance issued by the Secretary of State for Health and Social Care.
3.3.4 Approve the Trust’s policies and procedures for the management of risk.
3.3.5 Approve Final Business Cases for Capital Investment schemes where the value exceeds £1,000,000.
3.3.6 Approve the Trust’s annual revenue and capital budgets.
3.3.7 Ratify proposals for acquisition, disposal or change of use of land and/or buildings.
3.3.8 Approve PFI proposals.
3.3.9 Approve the opening of bank accounts.
3.3.10 Approve proposals on individual contracts (other than NHS contracts) of a capital or revenue nature amounting to, or likely to amount to over £1,000,000 during the duration of the contract.
3.3.11 Approve proposals in individual cases for the write-off of losses or making of special payments above the limits of delegation to the Chief Executive and Director of Finance (for losses and special payments) previously approved by the Board.
3.4.1 Approve the process for approval, dissemination and implementation of policies.
3.4.2 Approval of policies is delegated to the Executive Directors however the Board shall maintain responsibility for approving the following policies:
3.5.1 Approve the appointment (and where necessary dismissal of External Auditors recommended by the Audit Panel).
3.5.2 Approve external auditors’ arrangements for the separate audit of funds held on Trust, and submission of reports to the Audit Committee meetings which will take appropriate action.
3.5.3 Receive the Auditors Annual Report from the external auditor and agree action on recommendations of the Audit Committee, where appropriate.
3.6.1 Receive and approve the Trust’s Annual Report and Annual Accounts
3.6.2 Receive and approve the Annual Report and Accounts for funds held on trust
3.6.3 Receive and approve the Trust’s Quality Account.
3.7.1 Receive Escalation and Assurance Reports from Chairs of Committees in respect of their exercise of delegated powers. The remit of each Committee is specified within the relevant Committee Terms of Reference available via the Trust’s website and staff intranet.
3.7.2 Continuous appraisal of the affairs of the Trust by means of the provision to the Board of reports from directors, committees and officers of the Trust as set out in management policy statements. All monitoring returns required by the Department of Health and Social Care and the Charity Commission shall be reported, at least in summary, to the Board.
3.7.3 Receive reports from the Director of Finance on financial performance against budget.
4.1 This Reservation of Powers to the Board document will be reviewed on an annual basis in conjunction with the annual review of Standing Orders, Standing Financial Instructions and the Scheme of Delegation.
| S/O Ref | Delegated Matter | Delegated To |
| SO 1.2 | Final authority in the interpretation of Standing Orders | Chair (As advised by Chief Executive and Director of Corporate Affairs) |
| SO 1 | Advice on the interpretation or application of the Scheme of Reservation and Delegation of Powers | Director of Corporate Affairs |
| SO 2.5.1 | Responsibility for the overall performance of the executive functions of the Trust in line with the requirements of the Accountable Officer Memorandum for Trust Chief Executives. | Chief Executive |
| SO 2.5.1 | Responsibility for the provision of financial advice to the Trust and supervision of financial controls and accounting systems and discharge of obligations under relevant Financial Directions. | Director of Finance |
| SO 3.2.4 | Public to be informed of the Board of Directors agenda at least three days before the meeting. | Director of Corporate Affairs |
| SO 3.6 | Responsibility for deciding whether a vote is required and what form this will take. | Chair |
| SO 3.14 | Review each decision to suspend Standing Orders | Audit Committee |
| SO 4 | Board of Director approval to establish and disestablish Committees of the Trust | Director of Corporate Affairs |
| SO 4.8 | Advise the Board of Directors on the selection and appointment of the External Auditor | Audit Panel |
| SO 5.2 | Use of emergency powers relating to the authorities retained by the Board of Directors | Chair & Chief Executive acting jointly (following consultation with 2 NEDs & 2 Voting Executive Directors) |
| SO5 | Preparation of a schedule for Decisions Reserved to the Board of Directors and Scheme of Delegation | Director of Corporate Affairs |
| SO 6 | Establish Register of Interests for publication on Trust website | Director of Corporate Affairs |
| SO 7 | Compliance with Standards of Business Conduct: Policy on Managing Conflicts of Interest, Gifts and Hospitality and Sponsorship. | Director of Corporate Affairs |
| SO 8 | The Common Seal of the Trust shall be kept in a secure place. | Director of Corporate Affairs |
| SO 8 | Authorise use of Common Seal | Chief Executive, Director of Finance Director of Corporate Affairs (or their designated deputies) |
| SO 9 | Approval of Partnership Arrangements – Memorandum of Understanding | Trust Management Committee |
| SFI Ref | Delegated Matter | Delegated To |
| SFI 2 | Audit | |
| SFI 2 | Responsibility to ensure adequate internal and external audit services are provided involving Audit Committee in the selection process | Director of Finance |
| SFI 3 | INCOME, BUSINESS PLANNING, BUDGETS, BUDGETARY CONTROL AND MONITORING | |
| SFI 3.1.1 | Compilation and submission of annual plan taking into account financial targets and forecast limits of available resources | Chief Executive |
| SFI 3.1.2 | Preparation and submission of income and expenditure budgets for approval by Board of Directors prior to start of financial year | Director of Finance |
| SFI 3.1.3 | Monitor financial performance against budget and plan and advise Board of Directors | Director of Finance |
| SFI 3.1.4 | Provision of information to enable budgets to be compiled | Budget Holders |
| SFI 3.1.5 | Budget holders to sign up to allocated budgets at the commencement of each financial year | Director of Finance See Annex 1 |
| SFI 3.1.6 | Provision of adequate training to all budget holders relating to financial management within the NHS | Director of Finance |
| SFI 3.2.1 | Responsibility for the delegation of the management of budget to permit the performance of a defined range of activities. | Chief Executive |
| SFI 3.3.1 | Devise and maintain systems of budgetary control | Director of Finance |
| SFI 4 | ANNUAL REPORT & ACCOUNTS | |
| SFI 4.1.1 | Preparation and submission of financial reports in accordance with the accounting policies, guidance and timetable prescribed by the Department of Health and Social Care. | Director of Finance |
| SFI 4.1.1 | Preparation and publication of Annual Report a public meeting. | Chief Executive |
| SFI 5 | BANK AND GOVERNMENT SERVICE ACCOUNTS | |
| SFI 5.1.2 | Responsibility for managing Trust banking arrangements following approval by Board of Directors | Director of Finance |
| SFI 5.2.1 | Opening of bank accounts | Director of Finance |
| SFI 6 | INCOME, FEES AND CHARGES AND SECURITY OF CASH, CHEQUES AND OTHER NEGORTIABLE INSTRUMENTS | |
| SFI 6.1 & 6.1.3 | Design, maintain and ensure compliance with income and expenditure systems for prompt banking of all monies | Director of Finance |
| SFI 6.1.4 | Responsibility for ensuring appropriate arrangements are in place for authorisation of contracts of service provision through NHS or non NHS income activities | Chief Executive |
| SFI 6.2.2 | Approval and regular review of the level of all fees and charges, other than those determined by the DHSC or by statute | Director of Finance |
| SFI 6.3.1 | Responsibility for debt recovery and associated procedures | Director of Finance |
| SFI 6.4 | Security of cash, cheques and other negotiable instructions | Director of Finance |
| SFI 7 | NHS SERVICE AGREEMENTS FOR PROVISION OF SERVICES | |
| SFI 7.1 | Responsibility for ensuring the Trust enters into suitable service level agreements (SLA) or contracts with service commissioners for the provision of NHS services. | Chief Executive as Accountable Officer See Annex 1 |
| SFI 8 | TERMS OF SERVICE, ALLOWANCES AND PAYMENT OF MEMBERS OF THE BOARD AND EMPLOYEES (Annex 1) | |
| SFI 8.1.2 | Board of Directors to be advised in respect of the Chief Executive, Executive Directors and Very Senior Managers. | Nominations & Remuneration Committee |
| SFI 8.4 | Responsibility for processing payroll | Director of People |
| SFI 8.5 | Authority to issue, variate and terminate contracts of employment in a form approved by the Board of Directors | Director of People |
| SFI 9 | NON-PAY EXPENDITURE | |
| SFI 9.1.1 | Level of non-pay expenditure to be prepared on an annual basis for approval by Board of Directors | Director of Finance |
| SFI 9.1.1 | Responsibility to determine level of delegation to budget managers | Chief Executive |
| SFI 9.1.2 | Agree and maintain a list of managers authorised to place requisitions for the supply of goods and services | Director of Finance |
| SFI 10 | External borrowing and investments | |
| SFI 10.1.3 | Preparation of detailed procedural instructions concerning applications for loans and overdrafts. | Director of Finance |
| SFI 10.1.5 | Authorisation of short-term borrowing with the authority of two members of an authorised panel and advise next meeting of the Board. | Chief Executive or Director of Finance |
| SFI 10.2.2 | Responsibility for detailed procedural instructions on the operation of investment accounts and the records to be maintained. | Director of Finance |
| SFI 11 | CAPITAL INVESTMENT, PRIVATE FINANCING, FIXED ASSETS REGISTERS AND SECURITY OF ASSETS | |
| Preparation of Capital Programme for approval by the Board of Directors | Director of Finance | |
| SFI 11 | Maintenance of asset registers as specified in the Capital Accounting Manual issued by the Department of Health and Social Care. | Director of Finance |
| SFI 11.4.2 | Approval of Asset control procedures (including fixed assets, cash, cheques and negotiable instruments and donated assets). | Director of Finance |
| SFI 13 | DISPOSALS AND CONDEMNATIONS, INSURANCE LOSSES AND SPECIAL PAYMENTS | |
| SFI 13.1 | Detailed procedures for disposal of assets including condemnations | Director of Finance See Annex 1 |
| SFI 13.2 | Preparation of losses and special payments procedure | Director of Finance |
| SFI 13.2.2 | Preparation of fraud response plan setting out action to be taken | Director of Finance |
| SFI 13.2.4 | Approval to write off losses and special payments in accordance with the Scheme of Delegated Financial limits | See delegated financial limits within SFIs |
| SFI 13.2.7 | Maintenance of Losses and Special Payments Register recording write off action. | Director of Finance |
| 13.2.7 | Reporting of all losses and special payments to the Audit Committee | Director of Finance |
| SFI 14 | INFORMATION TECHNOLOGY | |
| 14.1 | Responsibility for accuracy and security of the computerised financial data of the Trust. | Director of Finance |
| 14.1.3 | Responsibility for publishing and maintenance of a Freedom of Information (FOI) Publication Scheme, or adoption of a model publication scheme approved by the Information Commissioner. | Director of Strategy & Partnerships |
| 14.5 | Responsibility to undertake risk assessments to ensure risks to the Trust’s financial systems from the use of IT are effectively, identified, considered and appropriate action taken to mitigate or control risk. | Director of Finance |
| 16 | Funds held on Trust | |
| 16.1.1 | Corporate Trustee for the management of funds held in Trust | Director of Finance |
| 16.1.6 | Responsibility for maintenance of accounts and records for Trust funds | Director of Finance |
| 16.1.7 | Responsibility for day to day management and operation of the charity. | Director of Strategy & Partnerships |
| SFI 16 | Delegation of Charitable Funds Expenditure | Director of Finance (See Annex 1) |
| SFI 16 | Charitable Funds Annual Accounts | Director of Finance |
| SFI 17 | TENDERING AND CONTRACT PROCEDURE | |
| SFI 17 | Approval of competitive tendering awards and appoint of tender evaluation panel | See Annex 1 |
| SFI 17 | Waiver of Standing Financial Instructions | Director of Corporate Affairs, Director of Finance, Chief Executive (or their designated deputies) |
| SFI 17.3.4 | Reporting of waivers to Audit Committee | Director of Corporate Affairs |
| SFI 18 | GIFTS AND HOSPITALITY | |
| SFI 18.1.1 | To ensure staff are aware of the Trust policy on acceptance on gifts and other benefits in kind through Standards of Business Conduct Policy: Policy on Managing Conflicts, Gifts and Hospitality and Sponsorship. | Director of Corporate Affairs |
| SFI 19 | RETENTION OF DOCUMENTS | |
| SFI 19 | Compliance with Records Management – NHS Code of Practice | Chief Executive and SIRO |
| Compliance with Access to Health Records | Medical Director acting as Caldicott Guardian | |
| Compliance with Data Protection and Freedom of Information Acts | Director of Strategy & Partnerships in conjunction with SIRO | |
| SFI 20 | RISK MANAGEMENT | |
| SFI 20 | Responsibility for programme of risk management | Director of Corporate Affairs |
| SFI 20 | Annual Governance Statement | Chief Executive |
Annex A
| Authorisation of Purchase Requisitions (Revenue and Capital) | |
| >£1,000,000 | Board of Directors |
| Up to £999,999 | Chief Executive |
| Up to £249,999 | Director of Finance |
| Up to £99,999 | Voting Director |
| Up to £49,999 | Non-Voting Director including Area Directors & Director of Integrated Contact Centres |
| Refer to SFIs for all other levels. | |
| Requirement to obtain Quotes and Tenders (Revenue and Capital) | |||
| Value Range (Inc VAT) | Requirement | Contract awarded by | |
| Up to £11,999 | Budget holder discretion | N/A | |
| £12,000 to £29,999 | Minimum of 3 formal written quotations | Director | |
| £30,000 to FTS Threshold | Minimum of 3 formal tenders | <£1m Director of Finance | |
| Above FTS Threshold | FTS process must be followed and must be published on Find a Tender Portal | <£1m Director of Finance >£1m Board of Directors | |
| Refer to Annex A of SFIs for further details | |||
| Cabinet Office Spend Control >£20m | |
| Refer to Annex A of SFIs for details | |
| Contract and Service Level Agreement Sign Off | ||
| Value range (inc VAT) | Contract/ agreements which do not commit the Trust to expenditure over one financial year. | Contracts/ agreement which commit the Trust to expenditure over more than one financial year. |
| 0-£11,999 (annual aggregated value) | N/A | Director of Finance |
| £12,000 to £29,999 | Director of Finance, Delegated to Head of Procurement if contract award decision ratified. | Director of Finance |
| £30,000 to Procurement Act threshold. | <£1m Director of Finance | <£1m Director of Finance |
| Above Procurement Act threshold | <£1m Director of Finance >£1m Board of Directors | <£1m Director of Finance >£1m Board of Directors |
| Authorisation of Charitable Funds Expenditure | |
| Head of Charity | Up to £999 |
| Deputy Director of Finance Head of Technical Accounts Director of Strategy & Partnerships | From £1,000 to £2,499 |
| Director of Finance or Chief Executive | £2,500 to £49,000 |
| Charitable Fund Committee or Board of Directors on behalf of Corporate Trustee | >£50,000 |
| Condemnation and Disposal of Assets | |
| Post holder | Authorisation limits (including VAT) |
| Relevant Executive Director and relevant Service Line Head of Finance | Where the net book value is up to £2,499 (subject to informal quotations for disposal) |
| Director of Finance | Where the net book value is between £2,500 and £24,999, (subject to competitive quotations for disposal) |
| Trust Management Committee | £25,000 to £249,999 (Subject to formal tender action to disposal) |
| Board of Directors | Where the net book value is >£250,000, (subject to formal tender action for disposal) |
| Losses,write off and Compensation | |
| Board of Directors | Write-off individual non-NHS debts in excess of £10,000. Ex-gratia payments for loss of personal effects above £10,000 (up to a maximum of £50,000). Losses (including cash) due to theft, fraud, overpayment and others in excess of £10,000 (up to a maximum of £50,000). Fruitless payments (including abandoned capital schemes) in excess of £10,000 (up to a maximum of £250,000). Damage to buildings, fittings furniture & equipment and loss of equipment and property in stores and in use to culpable causes (e.g. fraud, theft, arson) or other in excess of £10,000 (up to a maximum of £50,000). |
| Chief Executive | Ex-gratia payments for loss of personal effects between £5,000 and £10,000. Losses (including cash) due to theft, fraud, overpayment & others between £5,000 and £10,000. Fruitless payments (including abandoned capital schemes) between £5,000 and £10,000. Damage to buildings, fittings furniture & equipment and loss of equipment and property in stores and in use to culpable causes (e.g. fraud, theft, arson) or other between £5,000 and £10,000. |
| Director of Finance | Write-off individual non-NHS debts up to £10,000. Ex-gratia payments for loss of personal effects between £500 and £5,000. Losses (including cash) due to theft, fraud, overpayment and others up to £5,000. Fruitless payments (including abandoned capital schemes) up to £5,000. Damage to buildings, fittings furniture & equipment and loss of equipment and property in stores and in use to culpable causes (e.g. fraud, theft, arson) or other up to £5,000. Compensation payments made under legal obligation (no limit). |
| Head of Technical Accounts | Write-off individual non-NHS debts between £11 and £100 |
| Financial services Manager | Write-off individual non-NHS debts up to £10 |
| Authorisation of Income Contracts/New Service Initiatives | |
| Postholder | Authorisation limits (including VAT) |
| Director of Finance | Up to £250,000 |
| Chief Executive | Over £250,000 |
| Deputisation: Postholders with delegated powers are able to assign their powers to a nominated deputy (agreed by relevant Line Director) in the event of planned absences. For unplanned absences, a similar procedure should be followed although a memorandum would be prepared by the absent post holder’s Line Manager. | |
| Remuneration and Conditions of Service | |
| Very Senior Manager (VSM) Pay arrangements Authorisation of all pay, benefits and grading issues for Directors subject to VSM pay arrangement and NHS England (NHSE) approvalRecommendation of non-contractual termination payments to the NHSE and Treasury for approvalApproval of costs incurred in relation to Directors subject to VSM pay arrangements, senior managers and other cases where the cost exceeds £50,000Approval of business cases for redundancy where the costs exceed £50,000Recommendation contractual terminations to the NHSE where costs exceed £100,000 | Nominations and Remuneration Committee |
| Jointly approve business cases for redundancy/premature retirement applications where ethe cost does not exceed £50,000 | Director of People and Director of Finance |
| Field | Value |
| Recommended by | Audit Committee |
| Approved by | Board of Directors |
| Approval date | 24 April 2024 |
| Version number | 0.5 |
| Review date | April 2027 |
| Responsible Director | Director of Corporate Affairs |
| Responsible Manager (Sponsor) | Head of Risk and Assurance |
| For use by | All our people |
| Version | Date of Change | Date of Release | Changed By | Reason for Change |
|---|---|---|---|---|
| 0.1 | December 2020 | – | J Taylor | New Policy |
| 0.2 | January 2021 | January 2021 | J Taylor | Amendments from Audit Committee |
| 0.3 | 1 April 2022 | April 2022 | J Taylor | Annual Review |
| 0.4 | February 2023 | April 2023 | S White | Annual Review |
| 0.5 | February 2024 | April 2024 | J Taylor | Annual Review |
Risk management is both a statutory requirement and a key element of good management and risk
management is everyone’s responsibility, with the principles of effective risk management forming an integral component of decision making at all levels.
The activities associated with caring for patients, recruiting our people (staff and volunteers), providing
facilities and services, and managing finances are all, by their nature, activities that involve risk. These risks are present on a day-to-day basis throughout the organisation and whilst it may not always be possible to eliminate these risks, they can be managed to an acceptable level by ensuring that risk management is embedded into day-to-day practice and the culture of the organisation so that appropriate risk-based
decisions are regularly made by managers and staff at all levels.
Effective risk management enables the Board of Directors to determine the extent of risk exposure it currently faces with regard to the achievement of its objectives. As a key component of the internal control framework, regular review and routine monitoring of this policy will also inform the Trust’s Annual Governance Statement.
The purpose of this Risk Management Policy is to define the approach taken by North West Ambulance Service NHS Trust (the Trust) in applying risk management to its decision making at all levels and the main objective is to establish the foundations for a culture of effective risk management throughout the organisation.
This policy sets out clear definitions, responsibilities, and process requirements to enable the principles and techniques of risk management to be applied consistently throughout the organisation.
The principles and techniques of risk management as defined in this policy should be fully integrated within the formal governance arrangements and decision making processes of the organisation. All our people are responsible for making sure that they are aware of the organisation’s aims and objectives and are empowered to make decisions to manage risks as long as those decisions are within the scope of their role and level of authority.
Where a risk is identified but cannot be managed without some significant change to the way the organisation operates, it must be escalated through the relevant line management structure. The Risk Management Policy applies to all areas and levels of the Trust.
It defines the basic principles and techniques of risk management that the organisation has decided to adopt and forms the basis of all riskbased decision making. All risk management activities in the Trust will follow the process described within this document to ensure a common and robust approach is adopted to risk management.
This section details those groups and individuals within the Trust that have specific responsibilities withregard to the Risk Management Policy.
The Board of Directors is responsible for providing strategic leadership to risk management throughout the organisation, which includes:
• Maintaining oversight of strategic risks through the Board Assurance Framework (BAF)
• Leading by example in creating a culture of risk awareness
The Audit Committee is responsible for reviewing the established and maintenance of an effective system of integrated governance, risk management and internal control across the whole of the organisations’ activities. The Committee will provide assurance to the Board of Directors that there are effective systems operating across the Trust.
The Chief Executive as the Accountable Officer is responsible for ensuring an effective system of internal control is maintained to support the achievement of the Trust’s strategic objectives. This includes:
• The establishment and maintenance of effective corporate governance arrangements
• Ensuring that this Risk Management Policy is applied consistently and effectively throughout the Trust
• Ensuring that the Trust is open and communicates effectively about its risks, both internally and externally
• Retaining sufficient professional risk management expertise to support the effective implementation of this Policy
The Director of Corporate Affairs is accountable to the Board of Directors and Chief Executive for the Trust’s Governance and Risk Management activities. With Executive responsibility for governance and risk management the Director of Corporate Affairs (with support from the Head of Risk and Assurance) provides a clear focus for the management of organisational risks and for coordinating and integrating all of the Trust’s risk management arrangements on behalf of the Board of Directors.
Members of the Executive and Directorate Senior Management Teams are responsible for the consistent application of this Policy within their areas of accountability, which includes:
• Maintaining an awareness of the overall level of risk within the organisation
• The management of specific risks that have been assigned to them, in accordance with the criteria set out in this policy
• Promoting a risk aware culture within their teams and in the course of their duties
Area Directors/ Assistant Directors/ Heads of Operations/ Service/ Area Consultant Paramedics are responsible for the consistent application of this Policy within their areas of accountability, which includes:
• Making active use of the Trust risk register and the processes described in this Policy to support the management of their service
• The management of specific risks that have been assigned to them in accordance with the criteria set out in this policy
• Promoting a risk aware culture within their teams and in the course of their duties
• Ensuring that as far as possible risk assessments carried out within their service are based on reliable evidence.
All of our people (staff and volunteers) are responsible for identifying and managing risks within their dayto-day work, which includes:
The basic principle at the heart of the Trust’s risk management approach is that an awareness and
understanding of risk should be used to inform decision making at all levels.
This requires not only the active engagement of all our people with risk management activity in practice, but also the integration of risk management principles and techniques within the formal governance
arrangements of the organisation.
This will ensure that major strategic, policy and investment decisions are made with a full and reliable
appreciation of the risks associated with them as well as any existing risks that those decisions may serve to mitigate.
The risk management process, which can be seen in Figure 1 below, involves the identification, analysis,
evaluation and treatment of risks. More importantly, the process provides iterative steps, which when taken in a coordinated manner can support recognition of uncertain events which could lead to a negative outcome and therefore allows actions to be put in place to minimise the likelihood (how often) and consequence (how bad) of these risks occurring.
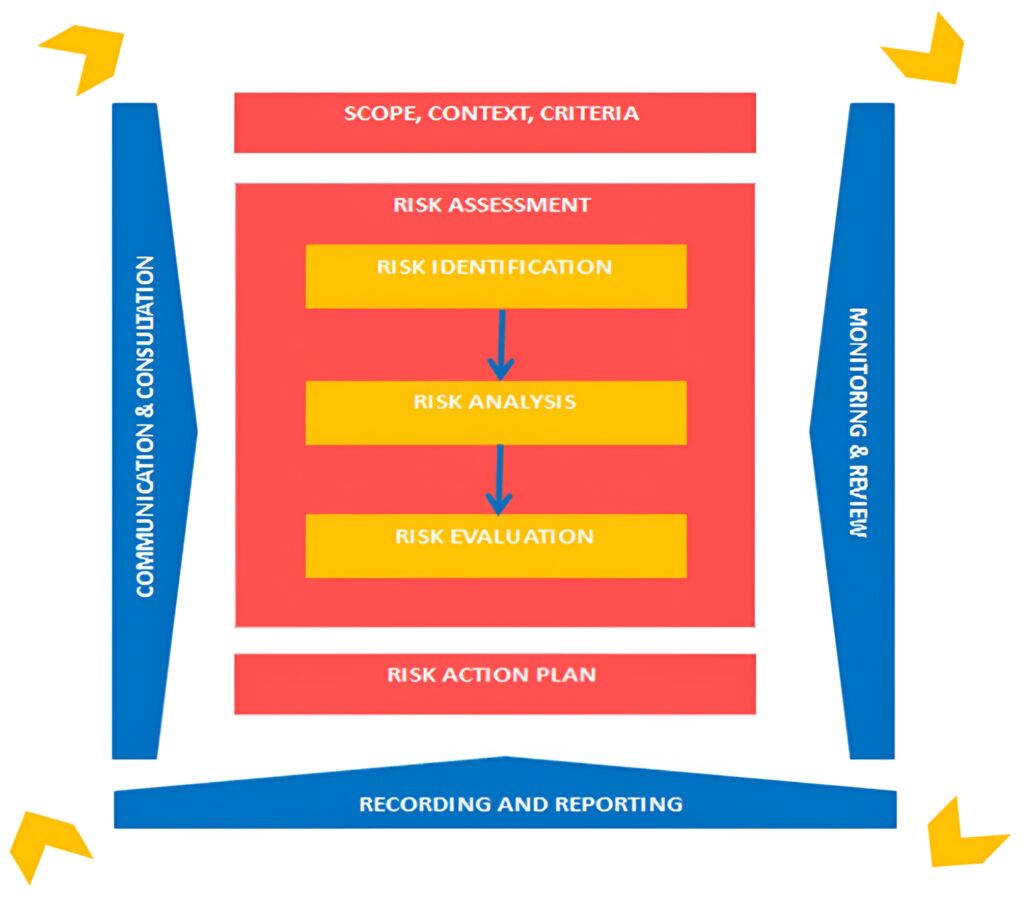
The Trust Strategy sets out our purpose to help people when they need us the most and a vision to deliver the right care, at the right time, in the right place; every time. This is broken down into 3 aims, these are:
Risks are linked to our aims because failing to control risks may lead to non-achievement of our strategic aims and/ or objectives.
Risk assessment is an objective process and where possible, staff should draw upon evidence or qualitative data to aid assessment of risk. Where evidence or data is not available, assessors will be required to make subjective judgement.
Risk vs Issue
It is important to understand the difference between a risk and an issue/ incident.
The fundamental difference between a risk and an issue/incident is that an issue/incident has already
happened, there is no uncertainty, and it is a matter of fact.
A risk is an uncertain event that has not yet happened, but if it did, it could affect the achievement of an objective.
| Risk | Issue / Incident |
| An uncertain event that HAS NOT happened | An unplanned event that HAS happened |
Risk Articulation
In order to assist the risk management process, it is essential that risks are described in a way that allows
them to be understood by all who read them. Articulating a risk in this way will enable effective controls, assurances and action plans to be put in place to mitigate the risk.
There should be three components to the description of a risk:
| Cause (Source of Risk) | Risk (Uncertain Event) | Consequence (Impact) |
| What has caused the risk? Where has the risk originated from? | The uncertain event (risk) that may happen if we do nothing | What would be the impact if the risk materialised? |
| Risk descriptions must tell a convincing story | ||
| There is a risk ‘as a result of/ due to/ because of’… existing condition Present Condition | An uncertain event… may occur Uncertain Future | Which would lead to… effect on objectives Conditional Future |
New risks and factors which increase a known risk may be identified at any time and by anyone within the organisation and can take many different forms.
All our people play a vital role in the identification of risk. All new risks should be reported and discussed with your line manager in the first instance, who will consider the best approach to manage the risk; this could be actions to immediately eliminate the risk, signposting of the risk to the appropriate person to manage the risk or inclusion on a risk register with an action plan in place.
Some risks can be managed effectively by the person identifying them taking appropriate action themselves or within their immediate team. This is particularly true with types of safety risk, where identification and removal of the hazard will often be sufficient to manage the risk.
Our people should initially consider what their main areas of work are and how these relate to their local objectives, and the objectives of the Trust. Every work activity that has a significant hazard should be assessed for risk. Identification using a systematic approach is critical because a potential risk not identified at this stage will be excluded from further analysis.
All risks, whether under the control of the Trust or not, should be included at this stage. The aim is to generate an informed list of events that might occur. Key sources that will inform this exercise include (but are not limited to):
• Compliance requirements with regulators and stakeholders such as the CQC, HSE, NHSE etc
• Recommendations from recent internal / external audit reports
• Thematic and trend analysis of incidents, inquiries, complaints, claims and inquests
• Performance data
• Quality Assurance Audits
• Quality Impact Assessments
• Safety Alerts
• Trend and forecasting analysis
• Risks associated with the achievement of corporate objectives
• Other methods of horizon scanning.
The NWAS Resilience Team work with partners in the Local Resilience Forums and Local Health Resilience Partnerships to examine National and Community Risk Registers and plan for multiagency risk mitigation and response. This is reviewed for the potential impact on the Trust, anything identified is recorded in accordance with this Policy and highlighted to the Emergency Preparedness, Resilience and Response (EPRR) Group, chaired by the Accountable Emergency Officer.
Recommendations from critical, major, or business continuity incidents and exercises are captured within the risk management processes to ensure the delivery of actions to reduce the risk of failure in the event of an actual incident.
Recommendations from thematic exercises from NHS Counter Fraud Authority (CFA) are captured within the risk management process to ensure the delivery of actions to reduce risk of failure in the event of an actual fraud, bribery, theft, and corruption incident.
The purpose of analysing and scoring a risk is to estimate the level of exposure which will then help inform how the risk should be managed.
When analysing a risk, you will need to:
• Identify who is affected and what is the potential consequence/ impact should the risk occur
• Estimate the likelihood (how often) the risk may possibly occur
• Assess and score the level of exposure to that risk using the risk scoring process below.
Risk Analysis Process
Risks are analysed using the Trust Risk Matrix. The Trust has adopted a 5×5 matrix with the risk scores taking account of the consequence and likelihood of a risk occurring.
The scoring of a risk is a 3-step process:
Step 1: Evaluate the consequence of a risk occurring. The consequence score has five descriptors:
| Table 1: Consequence Analysis | ||
| Score | Consequence Descriptor | Consequence Description |
| 1 | Insignificant | |
| 2 | Minor | |
| 3 | Moderate | |
| 4 | Major | |
| 5 | Catastrophic | Please see Appendix 2 for Consequence Descriptions |
Step 2: Analysing the likelihood (how often) a risk may occur. The table below gives the descriptions of the likelihood of a risk occurring:
| Table 2: Likelihood Analysis | ||
| Score | Likelihood Descriptor | Likelihood Frequency |
| 1 | Rare | Not expected to occur in years |
| 2 | Unlikely | Expected to occur at least annually |
| 3 | Possible | Expected to occur at least monthly |
| 4 | Likely | Expected to occur at least weekly |
| 5 | Almost Certain | Expected to occur at least daily |
Step 3: To calculate the risk score, multiply the consequence score with the likelihood score:
CONSEQUENCE score x LIKELIHOOD score = RISK score
| Likelihood / Consequence | 1 Insignificant | 2 Minor | 3 Moderate | 4 Major | 5 Catastrophic |
| 5 Almost Certain | 5 Low | 10 Moderate | 15 High | 20 High | 25 High |
| 4 Likely | 4 Low | 8 Moderate | 12 Moderate | 16 High | 20 High |
| 3 Possible | 3 Low | 6 Moderate | 9 Moderate | 12 Moderate | 15 High |
| 2 Unlikely | 2 Low | 4 Low | 6 Moderate | 8 Moderate | 10 Moderate |
| 1 Rare | 1 Low | 2 Low | 3 Low | 4 Low | 5 Low |
Once the risk analysis process has been completed, the risk score should now be compared with the level of risk criteria below which enables the Trust to measure the potential level of risk exposure and proceed to identify appropriate actions and management plans.
| Level of Risk | Range | Classification |
| Low | 1 – 5 | Low |
| Moderate | 6 – 12 | Moderate |
| High | 15 – 25 | High |
Each risk will be assigned 3 risk scores: initial, current and target. The risk scoring process above will be carried out three times for each score using the guidance below.
1. Initial Risk Score
The initial risk score is when the risk is first identified, the risk analysis process for initial risk scores should be a measure of the consequence and likelihood before any controls/ mitigating actions are proposed. The initial risk score will not change for the lifetime of the risk.
2. Current Risk Score
The current risk score, the risk analysis process for current risks should be a measure of the
consequence and likelihood once controls and mitigating actions are in place, taking into account the effectiveness of the controls added.
3. Target Risk Score
The target risk score, the risk analysis process for the target risk should be a realistic measure of the consequence and likelihood once improved mitigating actions have been achieved and improved controls added.
Effective risk management requires a reporting and review structure to ensure that risks are effectively identified, analysed and that appropriate controls and responses are in place.
Risk treatment is a process to modify risk and the selection and implementation of measures to treat the risk.
This includes as its major element, risk control/ mitigation, but extends further to the appropriate selection of a risk treatment option, these are outlined in the table below.
Can we accept the risk as it is i.e., without further controls? Would the
cost of controlling the risk outweigh the benefits to be gained?
Where the ability to do anything about certain risks may be limited or the cost
of taking any further action may be disproportionate to the potential benefit gained.
In these cases, the response is to manage the risk to as low as
reasonably practicable (ALARP) then tolerate the risk. This option can also be
supplemented by contingency planning for handling the consequences that
may arise if the risk is realised.
Where the status of the risk is to tolerate, the risk must be monitored and
reviewed by the risk owner at least annually. All risks tolerated, will be subject
to review by the Events and Risk Assurance Team and a decision made by the
Trust Management Committee if the risk should be tolerated or not.
Can we put controls in place to reduce the likelihood of the risk
occurring or its impact?
Treat is the most widely used approach and will be the course of action to take
for the majority of risks within the Trust before any other course of action is
considered.
Can we avoid or withdraw from the activity causing risk? Can we do
things differently?
A decision will be made by the Trust Management Committee if the risk should
be terminated or not.
Can we transfer or share, either totally or in part, by way of partnership,
insurance or contract?
This course of action should only be taken following consideration and
decision by the Trust Management Committee.
Controls are arrangements that are already in place to mitigate or manage the risk and these can include policies and procedures, monitoring, and audit.
Every control should be relevant to the risk that has been described, it should be clear that the control directly impacts on managing the risk and the strength of the control should be considered when deciding the influence this will have on the risk score.
Despite having identified controls, where the service has established a risk exists, it is the uncontrolled issues that are articulated as gaps. Gaps are issues which are not controlled and directly affect our mitigation of the risk. Gaps require clear and proportionate actions to address them.
Designed to limit the possibility of an undesirable outcome being realised. They
are important to stop an undesired outcome. It is crucial to implement these
types of controls.
For example, elimination of the hazard/ physically remove the hazard if
possible/ substitute with hazard with something less risky
Designed to limit the scope for loss and reduce any undesired outcomes that
have been realised. These may also provide a route of recourse to achieve
recovery against loss or damage.
For example, isolating people from the hazard, the use of guards, or barriers,
or reducing the exposure of the hazard
Designed to ensure that a particular outcome is achieved. This is based on
giving directions to people on how to ensure that losses do not occur. These
are important but depend on people following established safe systems of work.
For example, administrative controls such as changing the way people work,
training and supervision to enforce policies, procedures, processes, pathways,
use of Personal Protective Equipment (PPE)
Designed to identify occasions when undesirable outcomes have been realised.
Their definition, ‘after the event’ they are only appropriate when loss or damage
has occurred.
For example, monitoring and surveillance, such as closed-circuit television
(CCTV), smoke detectors, fire alarms.
Risk Mitigating Action Plans
The purpose of risk action plans is to document how the chosen treatment options will be implemented.
Information should include:
Differentiating between Controls, Gaps and Actions
To summarise:
Contributory Factors
Contributory factors are the influencing and casual factors that contribute to the identified risk.
These factors affect the chain of events and can be positive as well as negative, and they may have mitigated or minimised the outcome of the risk materialising. More than one contributory factor can be selected.
Risk Monitoring and Review
The monitoring process should provide assurance that there are appropriate controls and risk mitigating
actions in place. The frequency of ongoing monitoring and review depends upon the seriousness of the risk.
As a minimum, this must be:
| Current Risk Score | Review Timescales |
| 1 – 5 (Low) | Bi-Annually |
| 6 – 12 (Moderate) | Quarterly |
| 15 – 25 (High) | Monthly |
| Consequence Score | Review Timescales |
| 5 | Monthly |
A risk register is a centralised repository of identified risks that may threaten the delivery of services. A risk register should be live, dynamic, and populated through the risk assessment and evaluation process. The Datix Cloud IQ (DCIQ) Enterprise Risk Management (ERM) system is used by the Trust to record, manage and monitor risks throughout the organisation. Where risks cannot be immediately resolved, these risks should be recorded onto the Departmental/ Team Risk Register.
The purpose of the risk register is to:
The Trust aims to support staff throughout the organisation to manage risk at the most appropriate level in the organisation whilst ensuring that there is a clear process for risk to be escalated when necessary to ensure discussion, action, advice, and support can be provided.
All risk owners can escalate a risk for discussion, action, advice, and support via the risk record in the DCIQ system. The risk owner must clearly articulate the reasons for the risk escalation. The table below shows the team to Board escalation route.
The diagram below defines the ‘Assurance and Escalation Pyramid’ and demonstrates the route of
assurance and escalation takes.
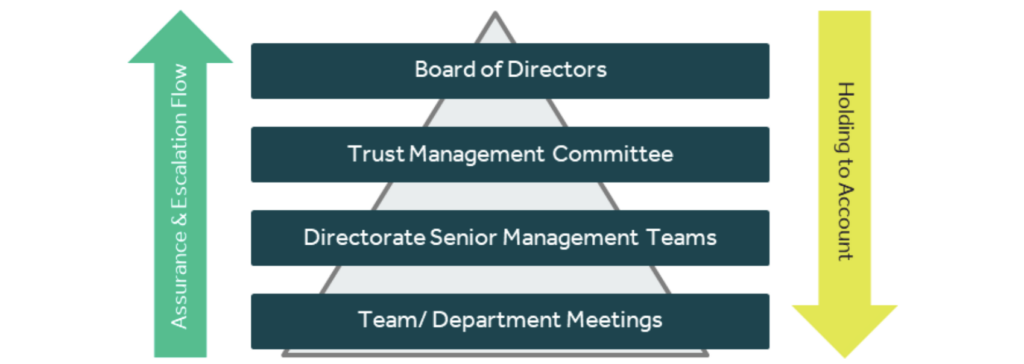
All risks held in the ERM Module in DCIQ scored 15 and above are automatically reviewed by the Events
and Risk Assurance Team. The below steps are followed to ensure the Trust Management Committee haveoversight of all high risks to the organisation.
Risks are overseen at various levels throughout the Trust as per the table below:
| Meeting | Type of Risk | Report Type | Risk Cycle |
|---|---|---|---|
| Board of Directors | Risks identified against delivery of strategic objectives | Quarterly Board Assurance Framework | As per Terms of Reference |
| Board Committees | Risks identified against delivery of strategic objectives relevant to their area of focus | Committee Board Assurance Framework Report | As per Terms of Reference |
| Audit Committee | Risks identified against delivery of strategic objectives | Quarterly Board Assurance Framework | As per Terms of Reference |
| Trust Management Committee | New & existing risk(s) scored 15 and above which indicate a high level of risk or where support is requested by the Directorates in the management of risk | Quarterly Board Assurance Framework Corporate & Commercially Sensitive Risk Register | As per Terms of Reference |
| Executive Led Groups | Visibility of risks scored 12 and above relating to the executive groups area of focus | Group Risk Report | As per Terms of Reference |
| Directorate Senior Management Team Meetings | Risks identified on the Directorate Risk Register | Directorate Risk Register | At least quarterly |
Directorate Senior Management Teams are responsible for exporting their own risk registers and ensuring risks on team/ departmental risk registers are being managed and reviewed in accordance with this Policy.
The risk reporting and assurance diagram highlights how the Trust aims to assure, scrutinise, escalate, and alert on risk management from front line to Board:
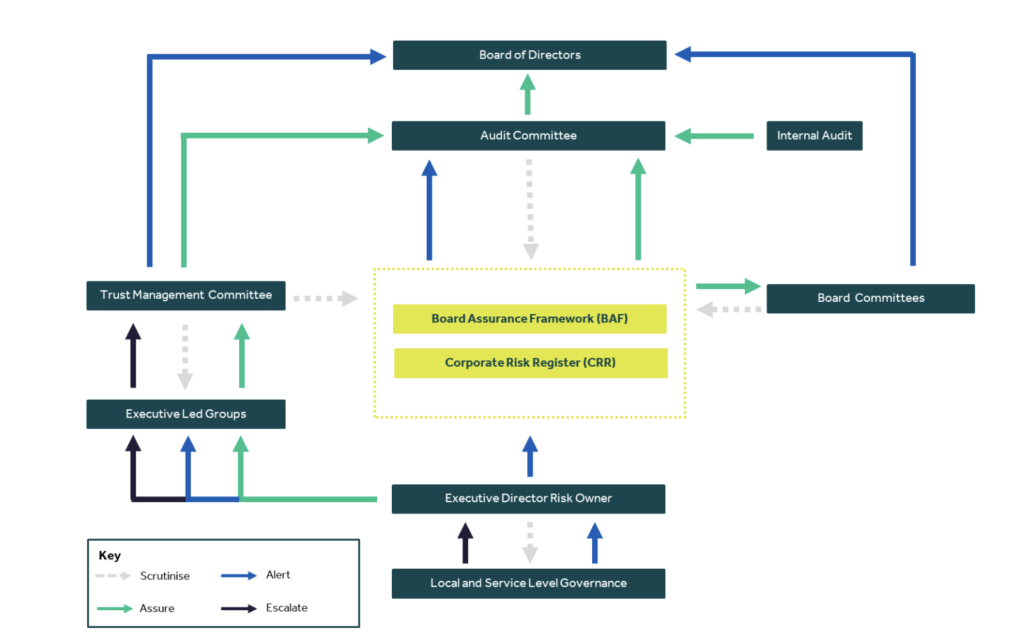
A key element of the Trust’s risk management system is providing assurance. Assurance provides evidence that risks are effectively managed by ensuring the effectiveness of controls and actions being put in place are making a positive impact and mitigating risks appropriately.
The Corporate Risk Register allows the Trust Management Committee to have oversight of risks where:
The Board Assurance Framework is a key document used to record and report the Trust’s key strategic objectives, risks, controls, and assurances to the Board of Directors. The Board Assurance Framework takes into account the recommendations from Audit, Executive Leads and Committees of the Board as to what should be included, amended, or removed. The Board Assurance Framework is updated and approved by the Board of Directors four times per year.
As outlined in the HFMA Audit Committee Handbook, the Audit Committee’s primary role in relation to the BAF is to provide assurance that the BAF itself is valid. The role of the Audit Committee is not to manage the processes of populating the BAF but to satisfy itself that the systems and processes surrounding the BAF are working as they should. This includes whether:
• The format of the BAF is appropriate and fit for purpose
• The way in which the BAF is developed is robust
• The objectives in the BAF reflects the Boards’ priorities
• Key risks are identified
• Adequate controls are in place and assurance are reliable
• Actions are in place to address gaps in controls and assurances.
Board Assurance Committees have the following responsibilities pertaining to the BAF risks pertaining to their areas of focus:
• Review of the BAF to ensure the Board of Directors receive assurance that effective controls are in
place to manage strategic risk;
• Report to the Audit Committee/ Board of Directors on any significant risk management and assurance Issues.
Executive Led Groups have the following roles regarding the operational risks pertaining to their areas of focus:
• Review the management of the operational risks (risks scored 12+) pertaining to their areas of focus;
• Report to the Trust Management Committee any significant risk management and assurance issues.
The Chief Executive is responsible for ‘signing off’ the Annual Governance Statement, which forms part of the statutory Annual Report and Accounts.
The organisation’s Board Assurance Framework gathers all the evidence required to support the Annual Governance Statement alongside the Head of Internal Audit’s annual opinion on the overall adequacy andeffectiveness of the organisation’s risk management, control, and governance processes.
Clinical risk management can be defined as:
“The continuous improvement of the quality and safety of healthcare services by identifying the factors that put patients at risk of harm and then acting to control/ prevent those risks.”
Clinical risk is identified through the analysis of patient safety incidents, clinical negligence claims, and complaints, identified areas of sub-optimal care, clinical audit and non-compliance with clinical policies, guidance, and training
The Executive Led Groups and the Audit Committee continually review and monitor all aspects of the Trust’s risk management system and play a key role in the standardisation and moderation of risks that are added to the Trust-wide risk register.
The Head of Internal Audit (HoIA) provides an annual opinion, based upon, and limited to the work carriedout to assess the overall adequacy and effectiveness of the organisations’ risk management, control, andgovernance processes.
Risk management guidance and advice are provided through the Corporate Risk and Assurance Team. Risk
management training is made available for staff, via MyESR as per the below table.
| Staff/ Group | Type of Training | Type of Delivery | Frequency of Training |
| All staff | Level 1 Risk Awareness Training | E-Learning | 3 Yearly |
| All staff who require access DCIQ Enterprise Risk Manager Module | DCIQ ERM Module Training | Virtually | Once |
| First line, Middle & Senior Managers | Level 2 Risk Management Training | E-Learning | 3 Yearly |
| Board of Directors | Level 3 – Risk Management and Assurance Training | E-Learning | Annually |
Taking into consideration the implications associated with this policy, it is considered that a target date of 01 April 2024 is achievable for communications about changes in this Policy, with any specific training being implemented on an ongoing basis. This will be monitored by the Trust Management Committee and the Audit Committee through the review process. If at any stage there is an indication that the target date cannot be met, then the Policy author will implement an action plan.
The Trust is committed to ensuring that, as far as is reasonably practicable, the way we provide services to the public and the way we treat our staff reflects their individual needs and does not discriminate against individuals or groups on any grounds. The Equality Impact Assessment can be viewed in Appendix 3.
Monitoring of compliance with this policy will be undertaken on a day-to-day basis by the Events and Risk Assurance Team, discussing any issues with the relevant team/ department/ Directorate and, if necessary, reporting to the Director of Corporate Affairs and relevant Executive Director Leads. The monitoring matrix can be viewed in Appendix 4 for further information.
This is an existing policy which has had moderate changes that relate to operational and/ or clinical practice and therefore requires a consultation process. The Head of Risk and Assurance has consulted with the Director of Corporate Affairs, Internal Audit and Local Counter Fraud to invite any comments or suggestions regarding this policy. The policy will be presented to the Trust Management Committee, Audit Committee and to the Board of Directors for approval.
Baker, T (2015). Board Assurance: A toolkit for health sector organisations. England: LLP
CQC (2010), Guidance about compliance; Essential standards of quality and safety. England: Care Quality Commission (CQC).
CQC (2023), Enforcement Decision Tree. England: Care Quality Commission (CQC).
Deloitte, Enterprise Risk Management Approach, A ‘risk-intelligent’ approach.
Good Governance Institute, Risk Appetite for NHS Organisations.
HMFA (2014). NHS Audit Committee Handbook. (3rd ed.). England: Healthcare Financial Management Association (MHFA).
Health Act 1999, Ch 8
Health and Social Care Act 2008, Ch 14
Health and Social Care Act 2012, Ch 7
Health and Social Care Act (Safety and Quality) Act 2015, Ch 28
Hopkin, P (2018). Fundamentals of Risk Management: Understanding, Evaluating and Implementing
Effective Risk Management. 5th ed. London: IRM.
Lark, J (2015). ISO 31000 Risk Management. (1st Ed). Switzerland: ISO
Moeller, R 2011). COSO Enterprise Risk Management: Establishing Effective Governance, Risk, and Compliance Processes. 2nd ed. New Jersey: Wiley & Sons.
NHS Providers (2018). Enterprise Risk Management.
PwC (2017). Delivering system wide sustainability: Managing risk in healthcare transformation. England: LLP.
The Orange Book: Management of Risk – Principles and Concepts, (2023). HM Treasury. London.
Vincent, C (2005). Clinical Risk Management. 2nd ed. London: BMJ Books.
| Term | Definition |
| Action | A response to control or mitigate risk |
| Action Plan | A collection of actions that are specific, measurable, achievable, realistic and targeted |
| Assessment | Means by which risks are evaluated and prioritised by undertaking the 4 stage risk assessment processes |
| Assurance | Confidence based on sufficient evidence that internal controls are in place, operating effectively and objectives are achieved |
| Board Assurance Framework | A document setting out the organisation’s strategic objectives, the risks to achieving them, the controls in place to manage them and the assurance that is available |
| Consequence (Impact) | The effect on the Trust if a risk materialises |
| Control | Action taken to reduce the likelihood and or consequence of a risk |
| Gaps in Control | Action to be put in place to manage risk and achieve objectives |
| Frequency | A measure of rate of occurrence of an event |
| Internal Audit | An independent, objective assurance and consulting activity designed to add value and improve organisations’ operations |
| Initial Risk | The score on identification before any controls are added |
| Likelihood | Evaluation of judgement regarding the changes of a risk materialising, established as probability or frequency |
| Mitigation | Actions taken to reduce the risk or the negative impact of the risk |
| Current Risk Score | The score with controls/ actions in place |
| Risk Appetite | The total amount of risk an organisation is prepared to accept in pursuit of its strategic objectives |
| Risk Matrix | A grid that cross references consequence against likelihood to assist in assessing risk |
| Risk Owner | The person responsible for the management and control of all aspects of individual risks |
| Risk Rating | The total risk score worked out by multiplying the consequence and likelihood scores on the risk matrix |
| Risk Register | The tool for recording identified risks and monitoring action plans against them |
| Risk Tolerance | The degree of variance from the Risk Appetite that the Trust is willing to tolerate |
| Strategic Risk | Risks that represent a threat to achieving the Trusts’ Strategic Objectives |
| Operational Risk | Risks which are a by-product of the day to day running of the Trust |
| Domain | Insignificant | Minor | Moderate | Major | Catastrophic |
| 1 | 2 | 3 | 4 | 5 | |
| Compliance: Legislative & Regulatory | No or minimal impact or breach of guidance/ statutory duty | Breach of statutory legislation | Single breach in statutory duty | Enforcement action, multiple breaches in statutory duty | Multiple breaches in statutory duty Inabolity to meet legislative requirements Breach of law Prosecution |
| Quality Outcomes | No/ minimal disruption/ impact to the provision of timely and accurate quality care Near-miss, no harm (physical and psychological) caused | Minor disruption/ impact to the provision of timely and accurate quality care Low physical/ psychological harm | Moderate disruption/ impact to the provision of timely and accurate quality care Moderate physical/ psychological harm | Severe disruption/ impact to the provision of timely and accurate quality care Severe physical/ psychological harm | Permanent loss/ inability to provide timely and accurate quality care Fatal |
| People | No injury or minor injury with no treatment required Aggression/ verbal abuse with minimal impact No staff sickness/ absence Temporary short term low staffing levels (less than 1 day) | Minor physical injury, illness or mental health illness requiring minor treatment Physical violence, assault, or verbal abuse with minor impact Short term staff sickness/ absence (less than 3 days) Insignificant staff attendance at mandatory/ key training (5%) Low staffing levels reducing service quality (1-5 days) | Moderate physical injury, illness, or mental health illness requiring hospital treatment Physical violence, assault, or verbal abuse causing moderate distress Staff sickness/ absence (more than 7 days) and/or RIDDOR reportable Poor staff attendance at mandatory/ key training (6-10%) Unsafe staffing levels (1-2 weeks) | Major physical injury, illness, or mental health illness requiring long term treatment or community care intervention Serious physical violence, assault, or verbal abuse leading to psychological harm Long term staff sickness/ absence Frequent poor staff attendance at mandatory/key training (11-20%) Unsafe staffing levels (> 1 month), loss of key staff | Fatality of staff member, life threatening injury, illness, or harm. Permanent injury, harm/ incapacity/ disability. Significant/ persistent low uptake of staff attendance at mandatory/ key training (>21% or 2 months+) Prolonged unsafe staffing levels, loss of several key staff, including industrial action |
| Finance | Small budget loss or claim between £0-£5k | Budget loss of 0.1- 0.25% or a claim between £5k-£10k | Budget loss of 0.25- 0.5% or a claim between £10k-£100k | Budget loss of 0.5- 1.0% or a claim between £100k-£1m Uncertain delivery of key objective Purchase failing to pay on time | Budget loss of >1% or a claim >£1m Loss of significant contract/ income. Non-delivery/ failu to meet key objective/ specification. |
| Reputation | Localised issue, ad- hoc public or political concern | Short term local media interest, reduction in public confidence and/or local political concern | Sustained local media interest, extending to regional interest, regional public and/or political concern with reduction in public confidence | Regional and/or national media interest with significant public and/or political concern and reputational damage | National media interest, parliamentary interest, public inquiry with loss of public confidence and credibility in NWAS |
| Domain | Insignificant | Minor | Moderate | Major | Catastrophic |
| 1 | 2 | 3 | 4 | 5 | |
| Innovation | Minimal or no loss of information containing identifiable data Cyber threat is expected to have negligible impact | Loss/ compromised security of one record containing identifiable data Cyber threat is expected to have limited impact | Loss/ compromised security of 2-100 records containing confidential/ identifiable data Cyber threat is expected to have serious impact | Loss/ compromised security of 101+ records containing identifiable data Cyber threat is expected to have severe or catastrophic impact | Serious breach with potential for identity theft/ compromised security of an application/ system/ facility containing identifiable data Cyber threat is expected to have multiple severe or catastrophic impact |
| Business/ Service | Interruption to provide NWAS services >1 hour | Interruption to provide NWAS services >4 hours | Interruption to provide NWAS services >6 hours Small-scale CBRN attack | Interruption to provide NWAS services >1 day Medium-scale CBRN attack Accidental fire Outbreak of emerging infectious disease | Prolonged/ permanent loss of NWAS service or facility Loss of critical system Terrorism Large-scale CBRN attack Major fire Pandemic |
| Programmes/ Projects | Temporary performance defects causing minor short- term consequences to time and quality | Project expectations not being met | Poor project performance shortfall in area(s) of secondary importance | Poor performance in area(s) of critical or primary objective | Significant failure of the project to meet its critical or primary objective |
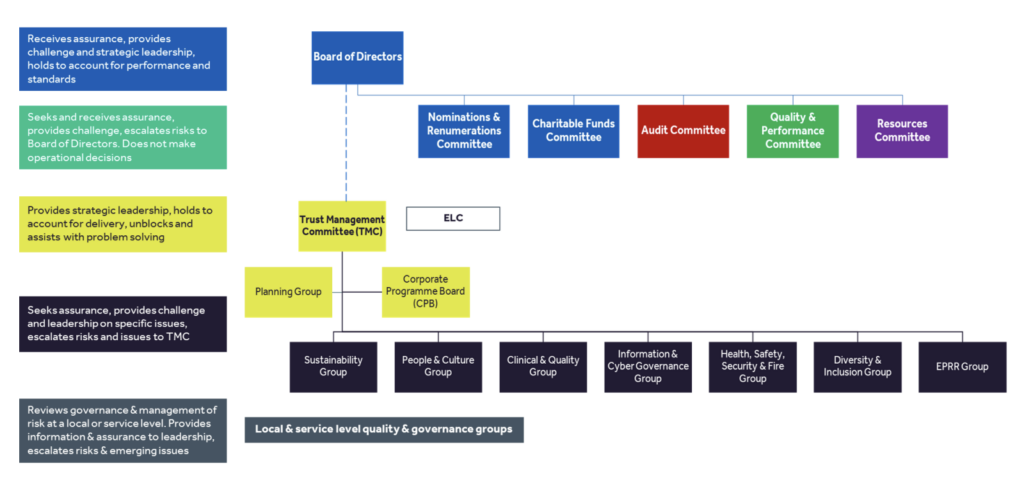
| Recommended by | Assistant Director – Operational Support Services |
| Approved by | OD Approval |
| Approval date | August 2023 |
| Version number | 3 |
| Review date | August 2026 |
| Responsible Director | Director of Operations |
| Responsible Manager (Sponsor) | Assistant Director – Operational Support Services |
| For use by | Volunteers and Volunteer Managers |
This policy is available in alternative formats on request.
Please contact the Human Resources Department on 01204
498400
| Version | Date of change | Date of release | Changed by | Reason for change |
| 0.1 | 13th July 2011 | 13th July 2011 | L Ward | Document creation |
| 0.2 | October 2011 | October 2011 | L Ward | Consultation with volunteer managers |
| 0.3 | May 2012 | May 2012 | L Ward | Feedback from Policy Group |
| 0.4 | June 2012 | June 2012 | E Forsyth | Feedback from EMT |
| 1 | June 2012 | June 2012 | E Forsyth | Approval |
| 1.1 | 3 April 2014 | 1st July 2014 | L Ward | Amendments following Francis Report Approval by Workforce & Communities Committee |
| 1.2 | February 2016 | March 2016 | L Ward | Review date |
| 1.3 | March 2016 | March 2016 | R Woods | Minor changes after policy group agreement. |
| 1.4 | May 2019 | June 2019 | Vickie Camfield | Review date |
| 1.4 | May 2019 | June 2019 | L Ward | Approval OD |
| 2 | Dec 2019 | December 2019 | L Ward | Policy Group and OD Approval for minor changes to responsibilities in section 11 |
| 3 | July 2023 | August 2023 | M Evans | Updates made that are aligned with current refences |
1.1 The purpose of this document is to set out the North West Ambulance Service
(NWAS) policy for including volunteers in its work and to set out the general
principles and guidelines for volunteering, to ensure consistent standards and good
practice.
1.2 In particular the policy will:
1.3 Volunteers provide a service to patients and their relatives. Their role is intended to
complement NHS services and it is not intended that they will be used as a direct
replacement for paid employment opportunities.
1.4 NWAS recognises the benefits of using volunteers including
2.1 The principles set out in this Policy apply to all individuals who undertake a volunteer
role directly on behalf of the Trust. Where NWAS has arrangements with third party
providers for the provision of voluntary support e.g., co-responder schemes,
individual volunteers will be covered by the host organisation’s policies.
2.2 A volunteer is defined as someone who commits time and energy for the benefit of
others, who does so freely, through personal choice and without expectation of
financial reward.
2.3 Volunteers are not employees and are not obliged to commit their time to NWAS. At
the same time NWAS is not obliged to provide opportunities for voluntary activities
when a volunteer is available. This means that any agreement with a volunteer is
binding in honour only and is not intended to form a contract. For clarity this means
that there is no entitlement to benefits such as sick pay or annual leave.
2.4 Staff may also act as volunteers, outside of their paid employment. Where the
voluntary role undertaken is different from their employed role, for example an
administrative member of staff undertaking Community First Responder duties, they
will be covered by this policy in terms of induction training and support. Reference
should also be made to the separate procedure relating to Staff Volunteers.
3.1 Volunteers may be used in a variety of ways in NWAS but the following are the most
frequent volunteering opportunities available:
4.1.1 The overall responsibility for the operation of a voluntary scheme lies with the
relevant line management in the responsible directorate. Managers will take
responsibility for ensuring that staff within their area are aware of the policy and any
specific arrangements for the use of volunteers in their area. They are also
responsible for inducting volunteers and providing ongoing support and monitoring of
their activities and ensuring that volunteers undergo an appropriate recruitment and
selection process and that they are safe to work with patients.
4.3.1 Staff are responsible for being aware of the policy and for recognising the valuable
contribution that volunteers can make to the quality of care offered to patients.
4.4.1 Volunteers are responsible for ensuring that they follow the guidelines in this policy
and any detailed guidance applicable to their Volunteering activity. This is often set
out in a memorandum of understanding which volunteers will be expected to sign to
indicate their acceptance prior to commencing voluntary activity.
4.4.2 All volunteers have a responsibility to take account of the Working Time Regulation
principals in terms of their overall working hours including their volunteer hours
5.1 Recruitment and selection processes in use for volunteers will be appropriate to the
voluntary activity being undertaken but in line with the guidance on the use of
volunteers issued by the Department of Health and consistent with the regulations
governing employment checks in the NHS. This requires that certain checks are
undertaken to ensure the safety of volunteers and staff engaged in direct patient
related activity. For example, this means that all volunteers engaged in patient
related activity will be required to undergo an enhanced Disclosure and Barring
Service (DBS) check, provide references and may be required to undergo some
health screening.
5.2 NWAS is however, mindful of the need to encourage volunteers from all sections of
the community and will proactively consider how volunteers are recruited and how
the recruitment and selection procedure can be adapted to recognise the voluntary
nature of the role. Recruitment will be conducted in line with the NWAS Equal,
Diversity and Inclusion Policy and the Recruitment and Selection Policy and
Procedure.
5.3 In line with national recommendations following the Saville review, volunteers
working undertaking patient facing voluntary activity with the Trust will be required to
undergo three yearly DBS check to ensure their continuing suitability to act in a
voluntary role.
6.1 All Volunteers will receive an induction which will provide background information
regarding the Trust, information about the activity they will be undertaking, the
standards of behaviour they will be expected to meet, key contacts, and any
administrative arrangements, such as how to claim expenses where these are
appropriate. Some of this information may be provided in the form of a Handbook (for
PTS Volunteer Car Drivers) or Memorandum of Understanding (for Community First
Responders) but it will always be supplemented by a personal induction from a
relevant member of staff from the directorate in which they will be volunteering.
6.2 Volunteers will be provided with any training necessary to carry out their volunteer
role. In most cases induction will be sufficient to meet the training needs of
volunteers but some voluntary activity, such as Community First Responder
schemes, will require specific training. In these cases, the local manager will be
responsible for ensuring that any relevant training is refreshed at appropriate
intervals.
6.3 Where appropriate volunteers may be issued with equipment to enable them to carry
out their voluntary activity.
7.1 Volunteers are not under any obligation to offer their time to NWAS and NWAS is not
under any obligation to use volunteers when they indicate that they are available. A
volunteer should never be coerced to give of their time as it must remain a free
choice for someone to offer to volunteer.
7.2 Obviously good communication between volunteers and NWAS is critical to ensure
that patients are not let down in the services we deliver. The specific arrangements
for advising NWAS of availability will vary between schemes and, where it suits
volunteers they will be able to indicate their availability in advance.
8.1 In some cases volunteers will be able to claim for actual expenses incurred. The
circumstances in which an expenses claim can be made will vary according to the
Volunteer activity and the details will be provided to volunteers during induction. The
following is not an exhaustive list but is indicative of the types of expenses that a
volunteer may incur and for which they may be able to claim reimbursement:
8.2 Volunteers will be advised of the relevant forms on which they can make expenses
claim. All claims will have to be authorised by an appropriate manager and volunteers
will be asked to provide bank details to enable expenses to be paid direct into their
bank accounts.
8.3 Volunteers should be aware that there is a mileage limit that volunteer drivers may
travel before they have to declare their income received through voluntary driving to
the HMRC. Once this limit is reached volunteers may be required to pay income tax
on some of their expenses. The limit varies and further information can be obtained
from the HMRC website.
8.4 In addition, any expenses received may be classed as income by HMRC or the
Benefits Agency and volunteers are advised to discuss their volunteer activities with
the relevant body if they have any concerns. NWAS is not in a position to provide tax
or benefits advice.
9.1 Managers must ensure that volunteers are supervised to an appropriate level and are
aware of whom to approach for advice and guidance if needed. Each volunteer will
be advised of the relevant manager or supervisor who can provide ongoing support
during the course of their voluntary activities.
10.1 Volunteers are representatives of the Trust and must always maintain a level of
professionalism and courtesy when dealing with patients and members of the public.
10.2 Volunteers are expected to be respectful of different customs, values, sexuality,
religion, belief, age or social background. Volunteers are expected to abide by the
general code of conduct provided in Appendix 1 and any more detailed guidance
provided in their induction.
10.3 Although volunteers are not employees they will be expected to follow relevant Trust
policies, such as those relating to infection control, patient confidentiality, health and
safety and equal opportunities. Relevant information will be provided to volunteers at
induction to ensure that they are aware of the standards they are expected to adhere
to when undertaking voluntary activity.
10.4 The NHS Constitution establishes the core principles and values underpinning the
delivery of NHS services in England. It establishes the responsibilities and values to
which all NHS organisations and those working for them should adhere, both in the
delivery of care and in their day-to-day activities in the workplace with colleagues,
patients and members of the public. The Trust fully adopts the NHS Constitution and
also sets out its own core values and guiding principles. All volunteers are expected
to familiarise themselves with the NHS Constitution and the Trust’s core values and
to ensure that their behaviours reflect these at all times when they are undertaking
voluntary activity and representing the Trust.
10.5 Where there is a complaint or issue raised about the conduct of a volunteer this will
be investigated by NWAS. The volunteer affected will be given the opportunity to
provide their version of events as part of the investigation. As there is no obligation to
offer any voluntary activity to a volunteer, it is highly unlikely that a volunteer’s
services will be used whilst an investigation is ongoing. Once the investigation is
complete the volunteer will be advised of the outcome and reasons for it. During any
investigation, a Welfare Officer will be assigned.
10.6 NWAS reserves the right to cease using a volunteer where their conduct is felt to fall
short of what is expected.
10.7 Staff Volunteers should be aware that their conduct as a volunteer could affect their
employment. This is where their conduct as a volunteer brings the Trust into
disrepute or their conduct substantially affects the employee’s capability to work or
indicates their unsuitability for their employed role. In these circumstances staff may
be dealt with under the Disciplinary Procedure for activities undertaken in a voluntary
capacity.
10.8 Where appropriate, volunteers engaged in patient facing activity may be subject to
enhanced Disclosure and Barring Service (DBS) checks at regular intervals during
their use as a volunteer. The requirement and frequency of such checks will be
identified in the MOU for the volunteer groups affected. Where a volunteer refuses to undergo a regular check then the Trust reserves the right not to utilise them as a volunteer.
11.1 It is recognised that there may be occasions when difficulties arise in the relationship
between either individual volunteer and NWAS management, including difficulties
relating to conduct or behaviour of a non-clinical nature between volunteers and
management or other employees of NWAS. As Volunteers are not employees and
therefore those NWAS investigative and disciplinary policies and procedures which
relate to employees and are designed to conform to employment law are not
appropriate for volunteers. Where either an NWAS employee complains about the
conduct or behaviour or a volunteer makes such a complaint about a NWAS
employee, the good practice recommended by Volunteering England will be followed:
11.2 The emphasis, wherever possible, will be on informal resolution.
12.1 The Trust has a responsibility to create an environment where individuals feel able to
raise concerns in confidence. If you become concerned about safety, malpractice or
wrong doing whilst undertaking voluntary duties for the Trust you have a
responsibility to raise these concerns. This includes concerns which may affect
patients, the public, staff or the organisation. Details of how to raise a concern can
be found in the Memorandum of Understanding for your voluntary role or in the
Trust’s Freedom to Speak Up Policy and Procedure which can be found on the
Trust’s intranet / Green Room or relevant Trust website.
13.1 This policy should be read in conjunction with other relevant NWAS policies such as
Equality, Diversity and Inclusion Policy and the Recruitment and Selection Policy and
Procedure. In addition, it has been developed in light of the following documents:
14.1 The Director of Organisational Development is responsible for the implementation,
monitoring and compliance with this policy.
14.2 The effectiveness of the policy will be monitored by review of occasions when there
are complaints raised by volunteers or where there are conduct issues with
volunteers. Issues will be reported by exception.
The following Code of Conduct sets out the basic expectations that NWAS has of volunteers
who are undertaking voluntary activity and representing the Trust. It should be read
in conjunction with any detailed guidance provided in connection with a specific
volunteer Scheme or provided at induction.
Volunteers must:
Be polite, courteous, tactful and professional, showing respect for all individuals
irrespective of their background.
Not share political or personal views which would not be representative of the Trust
Ensure that all patient related information is kept confidential in line with the Trust’s
Patient Confidentiality and data protection policies.
Only make expenses claims which are accurate and relate to genuine out of pocket
expenses, necessarily incurred in the course of voluntary activity. This includes
ensuring that where volunteers are transporting patients they do so by the shortest
and most practical route.
Maintain appropriate standards of dress and presentation.
Ensure that they meet the required standards of fitness to carry out a voluntary role
and inform NWAS where there has been a change in their health status which might
affect volunteering.
Ensure that they are fit to carry out voluntary activities when they have made
themselves available, this includes not being under the influence of alcohol or drugs.
Ensuring that their car is fit for purpose and meets infection control standards if it is
being used for voluntary activities.
Ensure that they meet road traffic legislation and requirements if using their car for
voluntary activities.
Not exceed the level of care for which they have been trained as this could place
patients at risk.
Ensure that they look after their own and patient’s safety at all times not contact the
media or respond to the media about their volunteering activities.
Not accept any offers of gifts, hospitality or gratuities from patients.
Adhere to the values set out in the NHS Constitution and Trust statement ensuring
that behaviours and conduct whilst representing the Trust reflect these values.
In 2016 the Care Quality Commission (CQC) published their report ‘Learning, candour and
accountability: A review of the way NHS trusts review and investigate the deaths of patients in
England’. It found that learning from deaths was not being given sufficient priority in many NHS
organisations and consequently valuable opportunities for improvement were being missed.
The report highlighted NHS organisations could do more to engage families and carers with
recognition that their insights are a vital learning source. In 2017, the National Quality Board’s
(NQB) ‘Learning from Deaths framework’ applicable to all NHS acute, mental health and
community trusts was published.
In 2018, the Department of Health and Social Care announced its intent to extend the principles
of the learning from death process to ambulances trusts. Under the auspices of the Association
of Ambulance Chief Executives (AACE), the National Ambulance Service Medical Directors
(NASMeD) committed to a formal process with the NQB to produce a national framework for the
sector.
The NQB ‘National guidance for ambulance trusts on Learning from Deaths: A framework for
NHS ambulance trusts in England on identifying, reporting, reviewing and learning from deaths
in care’ was published in 2019. It sets the national standards and requirements for ambulance
trusts to undertake a process of learning from deaths and makes a requirement that all
ambulance trusts formally develop and publish a Policy on Learning from Deaths. The North
West Ambulance Service Policy on Learning from Deaths commits the organisation to a process
of learning in order to improve the care delivered to our patients and reducing avoidable harm
and deaths.
North West Ambulance Service (NWAS) has a vision to deliver the right care, at the right
time, in the right place. These commitments are underpinned by a promise to provide highquality, inclusive care and to use learning to continuously improve the safety of our systems,
processes, and practices whereby the care we deliver is informed by a constant process of
review.
This Policy on Learning from Deaths sets out the practices that will be used within NWAS to
review and learn from the deaths of patients who had been under our care. This learning will
ensure we are able to protect future patients from avoidable harm, reduce unwarranted variation
and provide truly patient-centred care. This Policy is consistent with the national guidance for
ambulance trusts on learning from deaths and formally establishes the implementation of a
standardised and transparent approach to learning.
This policy goes far beyond a process of simply counting, classifying, and reporting deaths; it is
a commitment to supporting our journey towards providing an outstanding service to patients,
their families and carers.
This policy applies to all Trust staff, including volunteers.
Board of Directors
The Board of Directors has the accountability for the ownership of Learning from Deaths via the
approval of this policy and the commitment to ensuring sufficient resource is available to
facilitate learning across the organisation.
Chief Executive
The Chief Executive has overall responsibility for ensuring a Learning from Deaths process in
place within the trust and for meeting all internal and external reporting requirements. The
Chief Executive will delegate this responsibility to the Executive Medical Director.
Executive Medical Director
The Executive Medical Director has ownership of the policy on behalf of the Chief Executive.
They will ensure that any changes in legislation or national guidance relating to Learning from
Deaths are made known to the Executive Leadership Committee and the Board of Directors via
the Quality & Performance Committee.
Executive Directors
It is the responsibility of Executive Directors to ensure compliance with this policy within their
area of control, to monitor all relevant learning resulting from the learning from deaths process
and ensuring that any recommendations regarding actions are implemented.
Consultant Paramedic (Medical Directorate)
It is the responsibility of the Consultant Paramedic (Medical Directorate) to provide professional
clinical advice and guidance with regard to the learning from deaths process and ensure reports
are completed in order that learning is disseminated and actioned within the organisation.
All Senior Clinicians and Managers
It is the responsibility of senior clinicians and managers to ensure this policy and associated
procedures are implemented within their areas of responsibility and to participate fully with the
review process in a timely manner. All senior clinicians and manages will commit to providing
feedback to their staff on the review process and subsequent learning. Senior clinicians and
managers have the responsibility to provide assurance to their management team on the
progression and quality of case reviews.
All employees
It is the responsibility of all employees, and volunteers where necessary, to participate in the
learning from deaths process promptly, openly and honestly.
Our policy on Learning from Deaths is an integral part of informing and developing the safest
possible systems for the delivery of care to our patients. In establishing a robust methodology to
learn from deaths, and in particular to determine whether harm has occurred during the final
episodes of life, we have enabled the opportunity to evolve our systems of care to deliver
against our core purpose to save lives and reduce harm. This policy challenges the organisation
to scrutinise the care we deliver to patients who die within our care. NWAS must identify
suboptimal care which reaches the patient because of something we should have done but
didn’t, or something we did do but shouldn’t have; it challenges us to get better and supports the
identification of areas for improvement.
We have adopted a process of structured judgement review in order to systematically and
consistently scrutinise the care provided to patients and therefore use the opportunity to
increase safety and reliability as well as promote the adoption of improvement methodology to
make real changes to practice.
This policy contributes to the systems and processes already established within the Trust and
whilst it formally commits the organisation to a process of learning from deaths which occur
whilst patients are within our care, it serves to augment organisational learning and compliments
the established clinical governance, patient safety and quality improvement procedures including
those around the Patient Safety Incident Response Framework (PSIRF) and clinical audit.
This policy seeks to strengthen and develop our partnership approach to information sharing
and joint learning. We recognise that opportunities for system-based learning should be actively
sought and that working in isolation is detrimental to patients. We will work with our partners
across the healthcare system in the North West to proactively share information and collaborate
with the aim of supporting system level and cross-agency learning and improvement in
accordance with the PSIRF principles. This is not a new commitment, but through the
implementation of this policy we will seek to formalise the arrangements we currently have with our partners and commit to a central role within the health system of the North West in learning
from the deaths of patients in our care.
In the emotive period following bereavement, this Policy makes a commitment to family
members, carers and loved ones that we will apply a genuinely empathetic approach to listening
to concerns and communicating openly with them throughout.
This Policy on Learning from Deaths aligns with the definitions and recommendations within the
National Framework for NHS ambulance trusts in describing the scope for patients considered
as appropriate for case record review. However, it is clear that this does not mean that all deaths
in scope must be reviewed. Section 7 articulates how we will determine of those cases that are
eligible for consideration, which ones will be subject to a review. Hence, the deaths that are
initially in scope are as follows:
Determining which deaths should be reviewed
In accordance with the national framework, not all deaths in scope must be or will be reviewed.
A two-tier process of selection to determine which cases are selected for case record review will
be utilised which is both recommended within the framework and appropriate to ensure
maximum benefit for organisational learning within NWAS.
The national guidance stipulates that the Trust must review all deaths where ambulance service
personnel, other health and care staff, and / or families or carers have raised a concern about
the care provided, including concerns about end-of-life care. This includes any concern raised
that cannot be answered fully at the time or anything not answered to the satisfaction of the
person raising the concern. These notifications, and the subsequent review, investigation, and
management fall under the Trust’s Patient Safety Incident Response (PSIRF) Policy as detailed
in Section 10.
In addition, the Trust will review a sample of each of the four categories listed below.
− Deaths of patients assessed as requiring category 1 and category 2 responses where there
has been a delayed ambulance response.
The Trust will determine a number across the four identified categories listed above which would
equate to 40 to 50 case reviews per quarter; this sample size produces a rich source of
information on care quality and on problems in care (Royal College of Physicians, 2016).
It is these reviews that this policy pertains to, with the Learning from Deaths methodology
providing a bespoke and comprehensive review of the sample incidents.
Deaths of Patients with Learning Disabilities
The Trust must report all deaths of those aged over four with a known learning disability to the
Learning Disabilities Mortality Review (LeDeR) Programme. The Trust will contribute to their
review processes when approached and share its review findings with LeDeR when relevant.
The Learning Disabilities Mortality Review programme is aimed at reviewing all cases of death
of an adult or child with learning disabilities, to identify any factors associated with that death
that may have been preventable, and to learn from them. Where it is known or suspected that
that an adult or child has a learning disability and has undergone a diagnosis of death, or
termination of resuscitation, then details of the learning disability must be recorded on the
Diagnosis of Death form and reported to the Support Centre for formal reporting. The Trust
commits to participating fully in LeDeR programme reviews when approached to do so.
Maternal and Neonatal Deaths
Maternal deaths will be reported to the Healthcare Safety Investigations Branch (HSIB) and the
Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK
(MBRRACE). The Trust’s Resuscitation (Diagnosis of Death) Policy should be followed for all
maternal deaths.
Neonatal deaths are managed in line with the guidance and processes detailed within the
Trust’s Sudden Unexpected Death in Infancy, Children and Adolescents (SUDICA) procedures
which includes formal notification to partner agencies.
The Trust will contribute to HSIB, MBRRACE and SUDICA review processes through this
information sharing process and will, when approached, contribute to reviews and investigations
and share its review findings when relevant.
Paediatric Deaths
The Child Death Review Statutory and Operational Guidance outlines the Trust’s statutory
duties with regards to notification and information gathering. The Trust will participate in child death review meetings, including Child Death Overview Panel (CDOP) meetings, whenever notified. In the event of a sudden unexpected death in a patient under 18 years, the Trust’s Sudden Unexpected Death in Infants, Childhood or Adolescents (SUDICA) procedures for the management of these incidents including the involvement of the police and partner agencies will be followed. Attendance at Child Death panels may be required, and this governance resides under the Trust’s Safeguarding Team.
Safeguarding Concerns
Any deaths where there are safeguarding concerns (either adult or child) should be referred to
the Trust’s Safeguarding Team or Head of Safeguarding (Head of Clinical Safety) in line with our
statutory duties. The Safeguarding Team has the responsibility for the liaison with partner
agencies and for facilitating Trust involvement in any subsequent review processes.
Deaths in Custody
These deaths fall under the relevant police forces’ remit; the Trust will participate and contribute
to any formal reviews arising from deaths in custody whenever approached.
There may be cases, in addition to reporting provisions listed above, when the Trust will make
the decision to conduct our own review of the death in addition to the formal, national process.
This is likely only to be applicable if we identify at early stage that there are potential learning
improvement actions which need to be taken in advance of the national review process to
prevent reoccurrence or further harm. However, this is discretionary and will always be in
addition to the Trust’s requirements to notify and contribute to the national review programmes
of the death.
The Trust will consider each case individually in order to determine whether it should also
undertake a review in each circumstance and will consider its decision to undertake an
independent review of these deaths in discussion with the relevant review programme, to
minimise duplication
NWAS utilises a structured method of case review for those deaths identified for inclusion
utilising a standard methodology based upon an adaptation of the Royal College of Physicians’
Structured Judgement Review process. The objective of the structured judgement review
methodology is to look for strengths and weaknesses in the caring process, to provide
information about what can be learnt about the systems and processes in use where care goes
well and to identify points where there may be gaps, problems or difficulty in the care process.
In order to identify the strengths and weaknesses of individual patient contact episodes there is
a need to look at the full range of care provided to an individual; adopting this holistic care
approach allows for the nuances of individual cases and the outcomes of interventions to be
considered.
An important feature of this method is that the quality and safety of care is judged and recorded
whatever the overall judgement of the case and good care is judged and recorded in the same
detail as care that has been judged to be problematic; we commit to doing this. Evidence shows
that most of the care provided within the NHS is of good or excellent quality; there is much to be
learned from the consideration of high-quality care and these opportunities should not be
overlooked. By supporting the implementation of this methodology, the knowledge and
expertise gained will be transferable to other areas of reflection and review within the
organisation. The methodology could, for example, be used to rigorously assess the care
provided for people who have had a cardiac arrest and therefore enhance the organisational
learning we can derived from such cases in addition to those identified by the learning from
deaths process.
The structured judgement reviews for Learning from Deaths are undertaken by senior clinicians
within our organisation and the appropriate subject matter experts depending on each individual
case. We will commit to the necessary training for these individuals to provide a consistent and
standardised approach across the organisation. Following implementation of the structured
judgement reviews methodology and training there is the opportunity to use this acquired
expertise in other areas of the Trust’s investigation and learning processes; any decision for
further adoption of the methodology lies with the responsible managers and directors for those
processes.
NWAS has a commitment to develop and work on our culture to become a learning organisation;
this policy supports the aim of achieving this and contributes to our development as a learning
organisation through the processes highlighted.
In accordance with the NQB Framework requirements we publish quarterly Learning from
Deaths reports. These reports will draw upon learning from deaths data acquired in the previous
quarter and will be submitted to the Clinical and Quality Group, Quality and Performance
Committee and ultimately the Trust Board. Following approval Trust wide dissemination of the
reports will take place together with associate briefing documents to ensure learning is accessible to all clinicians and staff. The Area Learning Forums will be utilised as key vehicles to present and share reports and key learning ensuring the dissemination is embedded within the formal sharing arrangements within the Trust.
The Trust will commit to share learning from reviews and investigations through the National
Ambulance Risk and Safety Forum who will highlight trends to the National Ambulance Quality,
Governance and Risk Directors Group (QGARD).
This Learning from Deaths Policy enhances and compliments the NWAS Patient Safety Incident
Response Plan and Policy.
PSIRF supports organisations to use their incident response resources to maximise improvement, rather than repeatedly responding to patient safety incidents based on subjective thresholds and definitions of harm, from which new learning will be limited.
Some patient safety incidents, such as deaths though more likely than not due to problems in
care (that is, those meeting the Learning from Deaths criteria for investigation) all require a
Patient Safety Incident Investigation (PSII) to learn and improve.
Patient safety concerns identified at any stage of the Learning from Deaths process should be
escalated by the Consultant Paramedic (Medical Directorate) to the PSIRF Team. The concern
should be reported within the Events Module in the Datix Cloud IQ (DCIQ) system. All patient safety concerns must be reported via the DCIQ system, this also allows the notification to the NHS England, Learning from Patient Safety Events (LFPSE) system.
All reported patient safety concerns will be triaged and reviewed against the NWAS Patient Safety Incident Response Plan and Policy to determine the level of learning response. Patient safety incidents that meet a National Requirement or a NWAS Local Priority will require the completion of a pro-forma and will be presented to the Patient Safety Event Cases (PSEC) Group. The PSEC group will determine if the incident meets a National Requirement or a NWAS Local Priority and if a Patient Safety Incident Investigation (PSII) is required.
NWAS will ensure that our people who are affected by the patient safety incident will be afforded the necessary support and given time to participate in a patient safety learning response, under PSIRF. All NWAS leaders will work within our just culture principles and utilise other teams to ensure our people are supported. NWAS service lines will ensure processes are adopted so leaders work within the PSIRF principles to ensure psychological safety.
In addition to the statutory and legal requirements place upon us to contribute to and participate
in coronial processes, through the implementation of this policy we commit to strengthening the
relationships we have with Coroners across the north west region and proactively engage with Coroner’s Offices in order to both share learning and enhance the opportunity for learning for us
as an organisation.
Through this policy we will commit to embedding the learning and lessons learnt from Coroner’s
Hearings and conclusions and will implement a process of dissemination across the organisation
utilising the Area Learning Forums as a key vehicle to share learning with clinicians and staff.
Learning from Deaths reports will, where appropriate, contain significant learning from coronial
processes as an included section and key messages will be disseminated within the associated
briefing documents.
We recognise that proactive engagement with Coroners will strengthen professional
relationships; selected and appropriate learning that the Trust derives because of the
implementation of this policy will be shared with Coroner’s Offices where the learning will be of
interest from those incidents occurring within individual Coroner’s jurisdictions.
A culture of openness, transparency and candour is essential to improving patient safety. The
Trust’s established Duty of Candour Procedure will be used to guide the processes for the interaction with bereaved families and carers during reviews of cases identified. NWAS is committed to engaging in a meaningful and compassionate way with bereaved families and carers. They will be provided with a primary point of contact and consulted on how they wish to receive feedback following the process. This will include cases where a joint review is being undertaken and where a death has been referred to the coroner and will be the subject of an inquest.
The Trust also has a statutory and contractual duty to meet the NHS standards of the Duty of Candour wherever there has been a notifiable patient safety incident. Where a case review identified through the Learning from Deaths process identifies concerns, the initiation of the Duty of Candour process will be rigorously applied.
A greater voice to the bereaved families and carers will be established through engagement with the Trust’s Patient & Public Panel (PPP). The PPP have provided scrutiny of our learning from death processes and provided assurance that we are meeting the needs of the population we serve. Invited members of the PPP will contribute to the moderation of individual case reviews providing the vital family, carer and public perspective.
NWAS is committed in supporting our staff in the event of a death of family member, friend, colleague or patient. Occupational health provide staff with access to independent and confidential counselling and support to help them deal with work related and personal issues.
The Trust also provides a safe and robust Trauma Risk Management (TRIM) assessment service for any member of staff to access. The TRIM system is a post traumatic peer led risk assessment tool which aims to keep staff functioning after a traumatic event, such as a death of a patient, and provides information about personal resilience to staff and managers as well as identifying staff that may need specialised help. The Trust also has an extensive network of peer support / Blue Light Champions who are also available to provide a listening ear and signpost to further services where necessary.
Our commitment to staff is to have a just culture. The basis for this is a shared set of values in which our staff trust that all case reviews, and where applicable investigations, will result in a timely, fair and comprehensive process. Staff are assured that any actions, omissions or decisions that reflect the conduct of a reasonable person under the same circumstances will not be subject to inappropriate or punitive sanctions.
The Trust will present quarterly reports on the outcomes of the Learning from Death reviews to the Clinical and Quality Group, the Quality and Performance Committee and ultimately to the Board of Directors. Scrutiny will be provided via this established governance process and serve to ensure that this Policy and the associated processes are fit for purpose and delivering upon their intended aims.
The Trust will produce an annual summary of learning from deaths within its Quality Account. This will provide a consolidation of the quarterly reporting information together with a narrative analysis of learning and resulting key themes, actions taken and the outcomes of these.