



Annual report and accounts 2024-25 (3MB pdf)
Contents
- Foreword
- Performance report
- Overview
- Performance analysis
- Annual sustainability report
- The accountability report
- Corporate Governance report
- Directors’ report
- Statement of accountable officer’s responsibilities
- Statement of directors’ responsibilities in respect of the accounts
- Annual governance statement
- Remuneration report
- Staff report
- Parliamentary accountability and audit report
- Financial statements
Chair and CEO Foreword
We are very pleased to welcome you to our Annual Report 24/25 in which, as well as presenting our performance against our statutory obligations, we are delighted to showcase the many remarkable achievements of our staff and the organisation as a whole.
As an NHS trust which has a unique insight into people’s lives, we are acutely aware of the responsibility we have. People rarely contact us because something positive is happening – the babies we help welcome into the world maybe the only exception! Our callers are usually upset, in pain, scared and even angry. It is our job to not only use our clinical skills for their medical need but also to bring comfort, compassion, empathy and support. This is an honoured position and one that we are very proud of.
We have a workforce that shows unfailing commitment to the people we serve. From the corporate staff who keep the wheels turning in the background, to the welcoming, comforting voice on the phone and the welcome presence in someone’s home or at the scene of an accident. We are there.
Our patients frequently contact us to tell us their stories and to express their thanks and relief when we have turned up for them. It is a privilege to read these and pass them onto those on the frontline. We would like to take this opportunity to also pass on our thanks to our staff and volunteers. We never doubt your compassion and dedication to our patients and we are exceptionally proud of all of you.
This year has had its own challenges but we believe we were in a strong position to meet those, to learn from them and to make every effort to alleviate them where we can. No matter how well an organisation performs, there is always something new to learn, everything is open to change and improvement, and we are especially proud that NWAS is a trust that continuously strives to do this.
Despite a difficult winter, we ended the year with a 999-call pick-up mean time of just one second, consistently ranking us among the top two ambulance trusts in England. For our most serious, category one calls, this response is crucial when every second counts. We answered 97.8% of 999 calls within five seconds, maintaining one of the best performance records nationally. A remarkable achievement by all in our contact centres!
Our response to Category 1 calls – the most urgent – has improved and continues to show sustained progress. Encouragingly, response times for lower acuity Category 3 and 4 calls have also improved for the second year in a row, now reaching levels not seen since before the pandemic. While prioritising the most urgent calls is essential, we remain focused on improving the experience of all patients.
We know that not all of our patients need to go to hospital and that needlessly doing so, can cause unnecessary stress and further exacerbate their condition. We’ve strengthened partnerships with health and care providers to reduce hospital attendance and support care closer to home. While this ensures a better experience and outcome for the patient, it also helps us reach other patients in the community with more ambulances available to respond to them. By addressing more cases via telephone, emergency ambulances are prioritised for patients in more urgent need.
It has been the case now that for some time, hospital handovers remain a key challenge, affecting ambulance availability and this continues to be one of our priorities into the next year. While some areas of the ICBs have seen improvement, others continue to face delays. We’re actively working with system partners to reduce these pressures and improve patient flow, ensuring that our crews can be available to respond more quickly and safely.
In 24/25, we have invested in integrating our 999, NHS 111, and patient transport services (PTS) into a single, more efficient contact centre. Phases 1 and 2 were completed during the year, and Phase 3 was approved in January 2025. We’re now mobilising the final stage to embed the integrated contact centre model in 25/26.
This work has also had a positive impact on our 111 service, with a 33 per cent improvement in calls answered within 60 seconds compared to the previous year. Faster response times are key for caller satisfaction and also help to improve the call abandonment rate which has reduced by 10 per cent.
On average, NWAS answers just under 4,000 emergency 999 calls each day and while some of those are duplicate calls for the same incident or call backs, this is a significant number of people who are relying on us to come to their aid. These calls have resulted in 1.1m face to face attendances in the year, a reduction of only 0.3 per cent compared to 23/24.
In order to streamline our service delivery directorate, improve clinical supervision and structure with a robust management line, we undertook a leadership review. We appreciate that this was a challenging time for some but an improvement in our category one and two, the most seriously ill patients, bears witness to the success of this. This clear, management structure enables local teams to form meaningful relationships with system partners and offer senior clinical advice, and also provides further opportunity for clinical staff to develop and grow, which in turn, means a better service for our patients.
It was disappointing that the long waited announcement of the patient transport service tender process was not concluded in 24/25 as expected, and we recognise that this has left our PTS colleagues unclear about the future of our contacts in Merseyside, Cumbria, Lancashire and Greater Manchester. Our contract has now been extended to 31 March 2026 and we hope that there will be a positive outcome after this.
This year, we commissioned a PTS improvement programme of work, which was initiated in November 2025 and builds on the work delivered in the PTS financial improvement plan (2023- 2025).
The improvement programme is designed to deliver better outcomes and experience for patients and staff, alongside our contractual obligations and financial efficiencies. The work streams will deliver a modern-day logistics operation, set against the backdrop of a combination of increasing activity, increasing places of care and more stringent performance standards.
More than 1.4m patient journeys were undertaken by the service in 24/25, which is a decrease of 8 per cent compared to the previous year and it was great to see that more than 90 per cent of PTS patients reported that they had been treated with dignity, compassion and respect.
In 23/24, the report on the emergency service response to the Manchester Arena incident was published and key actions were required to comply with recommendations. Many of these were anticipated and work had already begun and this continued in 24/25.
There has been significant focus by the resilience team on the education and training of staff and in particular, those with commander responsibilities and the next year will see the launch and embedding of our new Incident Response Plan.
Since its launch in 2022, we have worked in line with our Trust Strategy, the main aims of this was to provide high quality inclusive care, be a brilliant place to work and to work together to shape a better future. We think we have made great progress and as this report was published, we are working to shape a new strategy which we hope to launch in 2026.
This would be timely as in the same year, we will celebrate 20 years since the merger of the previous North West ambulance services. We have come a very long way since then. We are more than an emergency responder and now have an active role in population health and addressing health inequalities, cementing our place as a proactive and patient focused NHS provider.
We are very proud of all we have achieved in 24/25, we hope that you are proud of us too. As always, we are keen to hear from you and to listen to your experiences. Listening is how we learn, and learning is how we improve.
Peter White Salman Desai KAM
Chair Chief Executive
Performance Report
The trust’s Performance Report has been prepared under direction issued by the Department of Health and Social Care Group Accounting Manual 2024/25 in accordance with Chapter 4A of Part 15 of the Companies Act 2006, as amended by SI 2013 No 1970. The Companies Act 2006 (Strategic Report and Directors’ Report) Regulations 2013.
The Accountable Officer is responsible for preparing the Annual Report and Accounts and considers taken as a whole they are fair, balanced and understandable.
Salman Desai KAM
Chief Executive
Date: 18 June 2025
Performance Overview
The purpose of the overview section is to provide:
- A statement from the chief executive officer providing an overview of the performance of the trust during 24/25.
- A statement of the purpose and activities of the trust, including a brief description of the business model and environment, organisational structure, objectives and strategies.
- A synopsis of the performance analysis and assessment of the trust’s progress towards delivering its objectives
- Details of the key issues and risks that could affect the trust in delivering its objectives and affect the trust in delivering its objectives.
- An explanation of the adoption of the going concern basis where this might be called into doubt.
Chief Executive Statement
I have been a proud member of North West Ambulance Service for many years, prior to that, I began my ambulance career as a paramedic in Greater Manchester. I now introduce the NWAS Annual Report for the first time as Chief Executive, a role I was honoured to take on in January of this year.
This report is a culmination of 12 months of challenges, achievements, successes and lessons learnt – far too many for me to mention here, so instead, I am going to focus on those who make our organisation what it is – our people.
Behind all of the projects, activity and highlights that you will read about in this document, are more than 7,000 dedicated, skilled and committed individuals. They work as a team, they work to ensure this trust is the best it can be and every day, I am immensely humbled by the compassion and dedication they show to our patients.
In addition to our staff, we also have the invaluable support of more than 1,200 volunteers. As community first responders, volunteer car drivers and members of our public patient panel, these individuals give up their free time to support our emergency and patient transport services and shape the decisions we make. We are exceptionally grateful for their time and commitment to the trust and our patients and cannot thank them enough for all that they do.
In addition, I would also like to express my thanks to the trade union representatives we work with. While on occasion, we may have differing views, we ultimately all have the same objectives which is to provide a quality service to our patients, and to ensure our colleagues work in an environment where they can develop, are treated fairly and their wellbeing is a priority.
Our staff are our most valuable asset and to retain skilled and experienced people, it is important that we invest in their development. For the third consecutive year, we have achieved the Gold Standard in the Employers Network for Equality & Inclusion’s (ENEI) Talent Inclusion and Diversity Evaluation (TIDE) accreditation. We are one of only 25 Gold Standard winners out of 185 global entries, from across 26 different sectors. With an overall score of 94%, we are the third highest ranked organisation out of all entries this year.
We are trained to deal with complex incidents but behind the clinical skills are human beings with thoughts and emotions. We recognise that some incidents can have a profound effect on our colleagues and so we have developed a portal to support them. This has significantly improved the way in which managers are informed when it has been identified that one of their staff may need support.
This, and other means of support were utilised following the tragic incident in Southport on 29 July when three little girls were fatally stabbed at a holiday club. I have spoken to many of the staff who responded to the incident and it is clear that these kinds of events stay with them for a long time.
Staff from Southport and others were recognised at our annual Star Awards in March, a sponsorship funded event which celebrates the great and the good in our organisation. Listening to the stories of the award recipients is extremely heartening – from a senior paramedic who established a care home education initiative to help prevent falls, to an emergency medical technician (EMT) who wanted to inspire young people in Blackpool to start a career in the service.
Our Mental Health team and colleagues in our call centres won a Mental Health Safety Improvement Award at the HSJ Patient Safety Awards. Their newly developed advanced questionnaire module allows for a timely upgrade and response to patients who have overdosed on high-risk drugs, and there is no doubt that the initiative will save lives. A great demonstration of how working together can make a difference.
This year, we also saw an EMT win a Pride of Cumbria award for her work in enhancing community resuscitation in the county. This resulted in the installation of 49 new accessible defibrillators in the county in areas identified as high risk.
An advanced paramedic secured the Exceptional Specialist Paramedic award at the Ambulance Leadership Forum Conference in 2024, for his role in developing a simulation newborn and maternity training initiative alongside colleagues at Liverpool Women’s Hospital – improving the clinical skills for ambulance crews who attend births.
All of these successes were achieved in addition to their day to day roles which is why I know that working for the ambulance service is not just a job to our people. It is a devotion to the care and health of our communities, and this is why I am proud to hold the position I do.
This report contains many stories such as these, and I do hope you find it interesting and inspiring. If you are interested in joining our NWAS family, as an employee or volunteer, take a look at our website.
Finally, in June 2025, we will bid a fond farewell to our Chair, Peter White. Peter was Vice Chairman and Non-Executive Director of NWAS for four years before being appointed as Chair. As a Non-Executive Director he held specific responsibility for performance and quality as well as leading on behalf of the board on EPRR (Emergency Preparedness, Resilience and Response).
Peter has been with us since 2014 and has been a supportive, committed and dedicated member of the Board during that time, seeing us through the pandemic, various and many improvements, chief executive and board appointments and many other memorable moments.
I have thoroughly enjoyed working with him and on behalf of all the executive team, wish him well in his new endeavours.
Salman Desai KAM
Chief Executive Officer
History of the Trust
North West Ambulance Service NHS Trust (NWAS) was established on 1 July 2006 and is one of the largest ambulance trusts in England. NWAS provides services to a population to over seven and a half million people across approximately 5,400 square miles in the communities of Cumbria, Lancashire, Greater Manchester, Merseyside, Cheshire, and Glossop in Derbyshire.
The trust employs 7,775 staff who operate from over 100 sites across the region and provide services for patients in rural and urban communities, coastal resorts, affluent areas and in some of the most deprived areas in the country. We also provide services to a significant transient population of tourists, students, and commuters.
The North West region is one of the most culturally diverse areas in England, with over 50 different languages spoken by members of the community. Consequently, we place considerable emphasis on equality and diversity and public engagement activities to ensure that our services are accessible to all members of the community.
A strategic focus is to collaborate with our integrated care systems (ICS) and integrated care boards (ICB) to support the delivery of public and population health agendas and urgent and emergency care services. We are the only regional NHS organisation in the North West that operates across five ICSs:
- Lancashire & South Cumbria Health & Care Partnership
- Cheshire & Merseyside Health & Care Partnership
- Greater Manchester Health & Social Care Partnership
- North East & North Cumbria ICS
- Joined Up Care Derbyshire (which includes Glossop)
Our shared purpose, vision and values
At NWAS, we are connected by a shared purpose; to help people when they need us most. We aim to achieve the best possible physical and mental health outcomes for each person who needs us. We will provide high-quality emergency care to save lives and make a difference to people with life-threatening illnesses or injuries. For those with less serious conditions, we will tailor our response to each person’s needs. This may include urgent clinical assessment, advice over the phone, referring them elsewhere or alternative transport for scheduled appointments.
Our shared purpose is to help people when they need us most. Based on this purpose, our strategy sets out our vision to deliver:
- Right care means that we will provide outstanding care that is safe, effective, and focused on the needs of the patient;
- Right time means that we will achieve all operational performance standards for our paramedic emergency service, NHS 111, and patient transport service;
- Right place means that we will provide care in the most appropriate setting for each patient’s needs, taking fewer people to emergency departments by providing safe care closer to home or referring people to other health and care pathways;
- Every time means that we will provide services which are consistent, reliable, and sustainable.
To deliver our vision, our values of ‘working together,’ ‘being at our best’ and ‘making a difference’” guide the behaviours that underpin all that we do. These values describe the ’how’ and set the expectations for staff to provide compassionate care and improve outcomes and experiences for our people, patients, and communities.
Our 2022-2025 Trust Strategy
Our Strategy 2022-2025, was developed following extensive engagement with staff, volunteers, patients and service users to understand the areas of focus, together with extensive analysis of performance data from each of our service lines which informed the strategic aims and objectives.
To enable the trust to deliver on its strategic aims and objectives we have implemented supporting strategies in the areas of Quality, People, Service Development, Sustainability, Estates and Fleet and Digital. All strategies specify our three-year measures of success.
At the end of 2024, we agreed to extend the current Trust Strategy by one year and work would be undertaken to develop a new trust strategy and supporting strategies during 25/26 for approval and launch in March 2026. The rationale for extending the timeline for production is to better align the strategic planning process and ensure a robust plan is in place that ensures both internal and external factors are considered, including changes in trust leadership structures and outcomes from the NHS ten-year plan.
Aims
Our three organisational aims provide a framework of what we will focus on between 2022-2025, to achieve our vision:
Aim 1: Provide high quality, inclusive care
We recognise there are health differences between groups in the communities we serve. We will listen to understand and make sure our services are accessible to everyone. We will work to prevent harm while using learning and research to continuously improve patient care and experience. To achieve this aim, we must create the conditions to provide care which is:
- Safe
- Effective
- Person-centred
Aim 2: Be a brilliant place to work
We will create an environment where our people feel happy and safe, have access to equal opportunities and are supported to be at their best. We will be a brilliant place to work by:
- Looking after our people
- Investing in our people
- Leading our people compassionately
Aim 3: Work together to shape a better future
We will work together to improve the services we provide. We will work with our partners and the public to find solutions which improve access, outcomes, and experience for everyone. We will work together to become more sustainable and have a positive effect on our communities and environment. To deliver this aim, we will work together, internally, with partners across the North West, and with communities to work towards:
- One NWAS
- One North West
- One future
Our commitment to equality, diversity and inclusion extends beyond the lifespan of the Trust Strategy. The board of directors refreshed its commitment to EDI in 2024 committing to delivery of the following priorities over the following three years:
- We will embed fair and inclusive recruitment and progression processes to improve the diversity of the workforce at all levels.
- We will educate and empower our workforce and leaders to promote a positive psychologically safe culture, to support a reduction in the experience of bullying, harassment, discrimination and an improvement in retention.
- We will reduce health inequalities for our patients.
Annual Planning
During 24/25 we introduced our ‘planning framework’ which outlined our approach to annual planning. The planning framework sets out an integrated and collaborative approach to planning. The framework describes our way of planning, that aims to support the trust to improve the quality of services and outcomes for patients and deliver key objectives included in the Trust Strategy. The framework includes a high-level timeline for developing the annual plan and regular engagement and collaboration with key stakeholders. Stakeholder workshops were scheduled at key decision points to ensure the annual plan for 25/26 is stretching but also feasible based on current resource and capacity.
Our Services:
Integrated Contact Centres (ICC).
Following internal reconfiguration of services, the ICC includes 999, NHS 111 and Patient Transport Service (PTS) Contact Centre.
999 emergency operations centres.
Emergency operation centres (EOC) receive and triage 999 calls from members of the public as well as other emergency services. EOC staff provide advice and dispatch an ambulance service to the scene as appropriate. The clinical hub (CHUB) is based within the EOC, assesses patients via telephone and provides the most appropriate care based on that assessment. This may be an ambulance (either emergency or urgent care), GP referral, referral to other services or self-care.
NHS111.
NHS 111 deliver services for the North West region and are major contributors to the delivery of integrated urgent care. We signpost patients to the most appropriate care highlighted to them following triage and informed by the Directory of Services.
Patient Transport Services.
Patient transport services (PTS) provide essential transport to non-emergency patients in Cumbria, Lancashire, Merseyside, and Greater Manchester, who are unable to make their own way to or from hospitals, outpatient clinics or other treatment centres.
Paramedic emergency services.
Paramedic emergency service (PES) services are delivered by solo responders, double crewed ambulances and approved private providers who together deliver 999 emergency care for the population of the North West.
Resilience.
Our hazardous area response team (HART) and resilience teams are specially trained and equipped paramedics who provide a response to high-risk and complex emergency situations, including major incidents. They respond to major incidents to deliver our statutory responsibilities as a Category 1 responder under the Civil Contingencies Act 2004.
Volunteering.
We have one of the largest and longest-established community first responder (CFR) schemes in England, with CFRs operating across all areas of the North West, providing an effective, complementary service in their local communities.
We also offer several other volunteering roles, including Patient and Public Panel (PPP), Voluntary Car Drivers (VCD), Voluntary Car Service (VCS), Welfare Support Volunteers and Vehicle Movement Volunteers.
Corporate services.
As well as providing clinical services to patients, we provide a wide array of specialist, non-clinical corporate services. These wider teams offer a unique variety of services, for example, estates and facilities, communications, risk management, digital, vehicle maintenance, finance, and human resources.
Operational Performance during 24/25
During 24/25, 999 call demand fell by 0.7% compared with 23/24, with a total of 1,436,333 calls received with periods of variation due to external factors such as winter pressures. Patients were appropriately signposted by call handlers to alternative pathways rather than waiting for an ambulance response. A total of 1,118,433 emergency incidents were responded to during 24/25, a reduction of 0.3% overall compared to 23/24 due to multiple calls being received for the same incident, estimated time of arrival enquiries and telephone triage and signposting to more appropriate services.
Ambulance Response Programme
The Ambulance Response Programme (ARP) is a framework for ambulance trusts to deliver its service meeting the needs of its patients. The fundamental underpinning principle of ARP is to use the right resource at the right time, in the right place, all in line with our strategic aim. The delivery of ARP standards throughout 24/25 has been varied, with sustained improvements for high acuity category one calls, the most serious and life-threatening calls. Performance against category three and four also improved for the second year in a row, meaning that the response to those lower acuity calls is being provided quicker than any time since before the pandemic.
Response to category two calls increased, despite increases in deployed ambulance resources due to the increase in hospital handover times impacting on the availability of ambulance resources to respond to patients who need a face-to-face response.
A snapshot of our ARP performance during 24/25 is shown below:
| Ambulance response times | |
| C1 Mean (7 minutes) | 00:07:44 |
| C1 90th (15 minutes) | 00:13:11 |
| C2 Mean (18 minutes) | 00:29:49 |
| C2 90th (40 minutes) | 01:00:33 |
| C3 90th (120 minutes) | 04:19:49 |
| C4 90th (180 minutes) | 04:32:33 |
Table: ARP Performance 24/25
CQC Rating
We welcomed the CQC whilst they carried out a focussed inspection of Lancashire and South Cumbria Integrated Care System (ICS) and Cheshire and Merseyside ICS in 2022. The service lines included: emergency and urgent care, emergency operations centre and NHS 111. Whilst this was not a well led inspection, we have maintained our ‘Good’ rating.
| Safe | Effective | Caring | Responsive | Well-led | Overall | |
| Provider Wide | Good | Good | Good | Good | Good | Good |
| Emergency and Urgent Care | Good June 2020 | Good June 2020 | Good June 2020 | Outstanding June 2020 | Good June 2020 | Good June 2020 |
| Emergency Operations Centre | Good June 2020 | Good June 2020 | Good June 2020 | Good June 2020 | Good June 2020 | Good June 2020 |
| Patient Transport Service | Good Jan 2017 | Good Jan 2017 | N/A | Good Jan 2017 | Requires improvement Jan 2017 | Good Jan 2017 |
| Resilience | Good Nov 2018 | Good Nov 2018 | Good | Good Nov 2018 | Good Nov 2018 | Good Nov 2018 |
| 111 | Good Jan 2017 | Good Jan 2017 | Good Jan 2017 | Good Jan 2017 | Good Jan 2017 | Good Jan 2017 |
Table: CQC ratings.
In 2023, the Care Quality Commission (CQC) redesigned their assessment process and introduced a new system called the Single Assessment Framework (SAF). The CQC began to implement the SAF in the third quarter of 2023, however, full deployment was delayed following feedback and restructuring within the CQC.
During 24/25, North West Ambulance Service (NWAS) has continued regular, routine engagement meetings and enquiries with the CQC.
NWAS has actively worked on adapting and developing our own internal assurance processes in response to the CQC’s changes, ensuring evidence categories are measured, as set out by the CQC Quality Statements. NWAS will adapt as required, to ensure that as the CQC’s approach evolves, our own assurance processes evolve in parallel.
Statutory & Regulatory Financial Duties
We are required to achieve a number of statutory and regulatory financial duties. These are:
- Statutory duty to break even year on year and a regulatory duty to break even each and every year.
- Regulatory duty not to exceed the External Financing Limit set by the Department of Health and Social Care.
- Regulatory duty to contain capital expenditure, on an accruals basis, within approved Capital Resource Limits.
- Regulatory requirement to achieve the Capital Cost Absorption Duty.
- Regulatory duty to apply the Better Payment Practice Code.
In summary, for the 24/25 financial year, we achieved all of the statutory and regulatory financial duties.
In 24/25, our total income was £554.753m where income from patient care activities was £540.410m, the breakdown across these activities can be found within the Financial Review 24/25 on page 44.
Key Risks to Delivering Objectives
24/25 Strategic Risks
The key strategic risks during 24/25 were focussed on quality and patient safety, financial sustainability, operational performance, workforce, regulatory compliance, engagement with system partners, cyber security, reputation and achievement of strategic priorities and objectives.
The following list denotes the key strategic risks during 24/25:
- There is a risk that the trust does not provide high quality, inclusive care leading to avoidable harm, poorer patient outcomes and reduction in patient satisfaction
- There is a risk that the trust cannot achieve financial sustainability impacting on its ability to deliver high quality (safe and effective) services
- There is a risk that the trust does not deliver improved national and local operational performance standards resulting in delayed care and/or harm
- There is a risk that the trust will be unable to maintain safe staffing levels through effective attraction, retention and attendance of sufficient suitably qualified staff impacting adversely on delivery of performance standards and patient outcomes
- There is a risk that the trust does not improve its culture and staff engagement and this impacts adversely on retention and staff experience.
- There is a risk that non-compliance with legislative and regulatory standards could result in harm and/or regulatory enforcement action
- There is a risk that the trust does not work together with our partners in the health and social care system to shape a better future leading to poor effects on our communities and the environment
- There is a risk the trust suffers a major cyber incident due to persistent attempts and/or human error resulting in a partial or total loss of service and associated patient harm
- There is a risk that the trust attracts negative media attention arising from long delays and harm leading to significant loss of public confidence
- There is a risk that the that level of uncertainty and unpredictability both nationally and regionally impacts on, or results in, delayed achievement of our strategic priorities and objectives
Future 25/26 Strategic Risks
The key strategic risks during 25/26 will focus on quality and patient safety, financial sustainability, operational performance, workforce, regulatory compliance, engagement with system partners, cyber security, reputation and achievement of strategic priorities and objectives.
The following list denotes the key strategic risks identified for 25/26:
- There is a risk that if the trust does not provide the right care, at the right time, in the right place, this may lead to avoidable harm and/or poorer outcomes and experience for patients
- There is a risk that if the trust does not achieve financial sustainability, its ability to deliver high quality (safe and effective) services will be affected
- There is a risk that if the trust does not deliver against NHS net zero targets, it will impact on the trust’s ability to contribute towards environmental improvements and delivery of its Green Plan
- There is a risk that if the trust does not deliver improved sustained national and local operational performance standards across all services, patients may experience delayed care and/or suffer harm
- There is a risk that if the trust does not create an inclusive environment and look after its people’s wellbeing, safety and development, then it will be unable to attract, retain and maximise the potential of its workforce for the benefit of patients.
- There is a risk that a breach of legislative or regulatory standards could result in avoidable harm and/or regulatory action
- There is a risk that due to the geographical size of the trust it will be unable to effectively engage with its numerous system partners which may impact on its ability to achieve the medium-long-term plan
- There is a risk that if the trust suffers a cyber incident, it could result in an inability to deliver a service and associated harm.
- There is a risk that the recent planned changes around the board over the next 12 months could destabilise the organisation and impact delivery of strategic plans.
- There is a risk that due to the timing of contracting decisions for NWAS commissioned services (PTS and 111), this will impact the development of our strategic priorities and objectives
- There is a risk that the current financial landscape of the NHS may impact achievement of the trust’s strategic priorities and performance by reducing the availability of resources both financial and physical.
The Annual Governance Statement provides further information relating to how the NWAS Board of Directors maintain strategic leadership and oversight of risk management arrangements.
System Oversight Framework
NHS England’s System Oversight Framework provides the framework for overseeing systems and providers and identifies potential support needs. The framework is built around five national themes that reflect the ambitions of the NHS Long Term Plan, NHS People Plan and the shared local ambitions and priorities of individual ICSs:
- Quality of care, access, and outcomes
- Preventing ill health and reducing inequalities
- Finance and use of resources
- People
- Leadership and capability
As part of the NHS England’s oversight, performance is monitored across each of these themes whereby providers are allocated to one of four segments that identify the nature of support needs. Segment one reflects no specific needs and segment four reflects providers that require mandated intensive support.
NHSE has assessed the trust as being in segment two, which by default, all ICSs and trusts are allocated unless the criteria for moving into another segment are met.
Further information in relation to the System Oversight Framework can be found here: https://www.england.nhs.uk/nhs-oversight-framework/
Going Concern
After making enquiries, the NWAS Board of Directors has a reasonable expectation that the services provided by North West Ambulance Service NHS Trust will continue to be provided by the public sector for the foreseeable future and can realise its assets and discharge its liabilities in the normal course of business. For this reason, the directors have adopted the going concern basis in preparing the accounts, following the definition of going concern in the public sector adopted by HM Treasury’s Financial Reporting Manual. Detailed guidance in respect of going concern is set out in International Accounting Standard (IAS1) and the interpretation for the public sector context is set out in the Financial Reporting Manual (FREM) and the Department of Health and Social Care Group Accounting Manual (GAM) 2024/25. The trust’s Letter of Representation for 24/25 to Forvis Mazars LLP as external auditors refers to NWAS preparing its accounts on a going concern basis.
Working with ICSs and Partners
NWAS continues to work closely with ICB urgent and emergency care (UEC) teams, places, and providers across the North West to drive forward the UEC recovery plan.
In 24/25, a key strategic focus is our ongoing partnership with integrated care systems (ICSs) and integrated care boards (ICBs) to enhance the delivery of urgent and emergency care pathways and improve public and population health agendas. ICSs have successfully integrated NHS commissioners, health and care providers, and other partners to deliver patient-centred services tailored to the needs of specific populations.
While challenges remain in working across multiple ICS areas, NWAS has strengthened its position as a key partner in the urgent and emergency care (UEC) system. We continue to deliver UEC services on a large scale, providing valuable data and insights that help identify opportunities for improvement, promote shared learning, and drive best practice. Integrated care relies on collaboration between health and care providers to design services around patient needs, with a strong focus on preventing serious health issues and addressing inequalities. Our close working relationships within ICSs provide an opportunity to develop innovative solutions that ensure people receive the support they need when they need it most.
To maximise engagement and collaboration with stakeholders, we have made significant progress in enhancing NWAS’ role as a proactive, trusted partner. Through strengthened partnerships, we have embedded a culture of working together in a collaborative and forward-thinking way. Our evolving partner arrangements will further support system-wide integration, enabling us to work effectively and efficiently with stakeholders to achieve a unified approach.
The capital resource of the trust is managed as part of the overall capital envelope of the Lancashire and South Cumbria ICB. We have managed agreed capital resource of £29.851m with spend for the year in line with the resource.
The trust’s capital resources continue to be managed as part of the overall financial framework of the Lancashire and South Cumbria ICB. In 24/25, we have maintained a structured approach to capital investment, ensuring financial sustainability while prioritising key service improvements.
Our Partnerships and Integration team has continued to play a critical and pivotal role in strengthening relationships across ICSs with system partners. The team has built highly effective stakeholder relationships, embedding a culture of collaboration and shared goals. Working across traditional and new partnerships, they ensure a strong emphasis on integrated care that aligns with local places, populations, and systems. Each ICS area benefits from a dedicated Partnerships and Integration manager, working alongside NWAS’ directorate leadership teams and executive leads, to drive a collaborative and proactive way of working. This will continue going forward.
The Trust Strategy continues to set out our vision and priorities, ensuring alignment with system-wide goals. The annual planning process has been refined to facilitate delivery of our strategic objectives, underpinned by key priorities for 24/25.
As part of our commitment to continuous improvement, we will undertake regular reviews of the Trust Strategy to ensure it remains relevant and responsive to evolving internal and external factors. These reviews will help us identify emerging areas of focus and adapt our approach to meet the needs of the population we serve.
The Board Assurance Framework (BAF) provides an effective metric for oversight of the organisation’s strategic risks ie those which could prevent the trust from achieving its corporate objectives and links with the trust’s strategic aims, objectives, and vision. Further information regarding the effectiveness of the BAF can be found within the Annual Governance Statement.
Performance Analysis
Integrated Contact Centre (ICC)
Significant progress was made during 24/25 to integrate the patient transport services, 999, and 111 contact centre services into a fully integrated contact centre (ICC) is an ambitious and crucial initiative, for improving operational efficiency and patient care.
The proposals for the final structure of the integrated contact centre were approved in January 2025, and the project is in mobilisation stage. This final phase will be critical to completing the structural changes and embedding the integrated teams in 25/26.
Embedding the senior leadership team into the new structure is a key priority for ensuring that the integration is managed effectively. The continuation of embedding joint governance procedures is crucial to maintain consistency across all three services and ensure that integration happens in a structured, compliant, and efficient manner.
Across all areas, reductions in sickness and turnover indicate that the integration is having a positive impact on workforce stability. Increased positive feedback from staff surveys further reinforces the success of the integration progress so far. This is a key sign that the changes are not only benefiting the service at an operational level but also improving the workplace environment and culture.
111 calls answered
During 24/25 NHS 111 calls answered by NWAS for the North West fell by 19.6% when compared to the previous year. A significant factor in this was due to external support. This support allowed us to improve its workforce metrics such as reducing sickness and turnover rates, which directly contributed to better call handling and overall performance.
During 24/25, 83% of calls were answered within 60 seconds. This represents a 33% point improvement compared to the previous year. Faster response times are crucial for patient satisfaction and ensuring that urgent cases receive immediate attention.
With support, call abandonment rate reduced by 10%, a reduction to 2.7% in abandoned calls is a great achievement, showing that we are better equipped to handle the volume of calls, and fewer patients are left waiting or choosing to disconnect. Overall performance improvement for call pickup and workforce efficiency improved, which is in light of the recognition that the funded capacity in the north west is not sufficient to meet the demand of the service.
Support ceased in February 2025, whilst this has represented an increase in volume for the service, we have managed to maintain strong performance, especially for call abandonment (still within the target of under 5%).
999 call demand
In 24/25, 999 call demand has fallen by 0.7% overall compared with 23/24. However, there have been periods of variation based on external factors, for example winter pressures and a low call pick up mean (one second for the fiscal year). This means our patients are being more appropriately signposted by call handlers to alterative pathways, which in turn, reduces the number of subsequent calls received for the same patient who may have been waiting for an ambulance response.
| Fiscal year | 999 Call Demand | % difference to previous year |
| 21/22 | 1,632,595 | ↑ 26.7% |
| 22/23 | 1,531,958 | ↓ 6.2% |
| 23/24 | 1,446,700 | ↓ 5.6% |
| 24/25 | 1,436,333 | ↓ 0.7% |
Table: Total number of 999 calls (24/25) with percentage change from the baseline.
Figure: Average number of calls is 27,621per week, or 3,935 per day (24/25) with the reporting year highlighted in green.
The statistical process control chart shows a sharp rise in demand in the baseline year (August 2024) throughout the winter, where excess demand from seasonal flu, for example, increased demand across the whole NHS. The demand reduced in January 2025 and has been more stable in the first quarter of 2025, like the previous year.
Incidents requiring a response.
In 24/25, 999 emergency incidents requiring a response has decreased by 0.3% overall compared to 23/24. The number of incidents responded to is less than the number of 999 calls received for several reasons. These include multiple telephone calls being received for the same incident, estimated time of arrival enquiries and solving the patients’ needs through telephone triage and signposting to more appropriate services.
| Fiscal year | Emergency Incidents | % difference to previous year |
| 21/22 | 1,129,193 | ↓ 1.1% |
| 22/23 | 1,074,933 | ↓ 4.8% |
| 23/24 | 1,121,403 | ↑ 4.3% |
| 24/25 | 1,118,433 | ↓ 0.3% |
Table: Total number of 999 calls requiring a response (24/25) with a percentage change from the baseline.
Figure: The percentage of 999 calls answered shown weekly demonstrates increased consistency at or above 95% in 24/25.
Within the data, there are periods within the year where call pick up has dropped below the control limit on specific dates, for example July 2024 and November 2024, cause of which have been periods of high demand or business continuity events eg. unplanned loss of category three command and control system, meaning call handlers reverted to taking 999 calls on paper, which in turn increases call length, impacting performance. It is of note that we have finished the fiscal year 24/25 with a one second 999 call pick up average (mean) with NWAS continually being ranked in the top two NHS ambulance trusts nationally for call pick up.
In 24/25, 999 call pick up remained one of the best in the country with 97.8% of 999 calls answered within five seconds. Call pick up is a vital safety metric for patients with the most life-threatening conditions (category one) as cardiopulmonary resuscitation advice over the telephone is a critical success factor in survival.
| Fiscal year | % of calls answered in five seconds | % point difference to previous year |
| 21/22 | 75.9% | ↓ 19.1% |
| 22/23 | 72.8% | ↓ 3.1% |
| 23/24 | 96.8% | ↑ 24.0% |
| 24/25 | 97.8% | ↑ 1.0% |
Table: 999 Call pick up
Ambulance Response Programme
Ambulance service emergency performance is measured through the Ambulance Response Programme (ARP), which aims to make sure patients are reached as quickly as possible depending on their need. Under ARP there are four categories, with category one being the most serious, life-threatening incidents. All categories have a performance standard based on the time it takes to respond to the incident.
These performance standards can be seen below:
- Category one is for calls about people with life-threatening injuries and illnesses. We aim to respond to these in an average time of seven minutes and at least nine out of ten times within 15 minutes.
- Category two is for emergency calls. We aim to respond to these in an average time of 18 minutes and at least nine out of ten times within 40 minutes.
- Category three is for urgent calls. In some instances, you may be treated by ambulance staff in your own home. We aim to respond to these within 120 minutes at least nine out of ten times.
- Category four is for less urgent calls. In some instances, you may be given advice over the telephone or referred to another service such as a GP or pharmacist. We aim to respond to these at least nine out of ten times within 180 minutes.
- Category five – Signposting advice only, no response time apply.
Response to high acuity category one calls has improved in 24/25 and shows a sustained improvement over time. As these are the most serious and life-threatening of calls received, ambulance services prioritise their response to these patients to save lives.
There has also been improvement in the response to category three and four patients for the second year in a row in 24/25, meaning that the response to those lower acuity calls is being provided quicker than any time since before the pandemic.
Response to category two calls has increased in 24/25, despite increases in deployed ambulance resources. This increase has been driven by an increase in hospital handover times impacting on the availability of ambulance resources to respond to patients who need a face –to face response. Whilst the mean category two for 24/25 was just over one minute longer than 23/24, at 29 minutes and 49 seconds, it was still below the revised recovery target set by NHS England of 30 minutes. Work is underway to reduce the category two response time in 25/26 with additional investment expected from NHS England to allow the increase in frontline resources, further support to reduce handover times, and extra clinicians in the integrated contact centre to support the triage of calls.
During 24/25, we responded to slightly fewer incidents than the previous year. More incidents than ever before were managed without the need to transport a patient to hospital, with patients being provided care over the telephone, referred to another service (such as community pharmacy, community response, or their own GP), or managed at home with a face –to face response from an ambulance service clinician.
Hospital Handover
Arrival at hospital to handover of patient continues to be a challenge across our geographical footprint. The average amount of time it has taken for an ambulance crew to hand over the care of a patient to the emergency department staff after the arrival at the hospital has increased from 23/24.
We have seen a reduction in handover to clear times from those seen in 23/24 and have been consistently below 10 minutes each month on average for the whole year. This is the time taken after the patient is handed over to complete any paperwork and prepare the ambulance for the next emergency call.
Arrival to handover, and handover to clear, when taken together give us our overall turnaround time. The increase in the average arrival to handover time, with the small decrease in handover to clear time, means overall turnaround time has increased in the North West in the last 12 months. Some improvement has been seen in quarter four of 24/25 with significant focus on turnaround times by our integrated care board and NHS England partners.
Work continues closely with integrated care board partners, and with individual acute hospital trusts to improve handover. Over the last 12 months, we have deployed ambulance liaison officers to our busiest hospitals to help coordinate the release of ambulances, used cohorting (a process where one ambulance crew looks after a number of patients to free up other crews) to allow us make crews available for further calls, and teams have taken part in collaborative work with partners to review handover processes. This has delivered some success in the later months of the financial year – and it is expected that this work will continue into 25/26, to deliver handover times closer to the target of 15 minutes, and with a nationally mandated maximum time of 45 minutes.
Arrival to handover times are higher in Cheshire and Mersey than they are in the other integrated care board areas. There has been extensive engagement across the Cheshire and Mersey ICB area throughout the year to address this, including the development of several schemes to further reduce emergency department attendance and avoid long waits, and this is now starting to show some sustained improvement.
Releasing ambulances promptly on arrival at hospital increases the availability of ambulances and improves our capacity to respond to emergencies. This is why there has been significant focus from the leadership teams across NWAS, and from our integrated care board and acute hospital trust partners in reducing handover times.
All three areas of NWAS have been working with their respective ICBs around handover improvement. The three main North West ICBs all have a handover improvement working group, bringing together the acute hospitals, wider system partners, and senior leaders from NWAS to collaborate on handover improvement. These groups have been focused on improving flow through emergency departments to allow improvement in flow from waiting NWAS crews. Although the approaches have been different in the three areas, handover improvements have been delivered at some of the most challenged hospital sites in quarter four of 24/25.
Work has also been ongoing with the ICB in North Cumbria as part of some joint work between ourselves and North East Ambulance Service. This has focused on improving escalation when delays are experienced at acute hospital sites. Plans are in place to continue this work with all the ICBs into 25/26, supported by the NHS England regional team, with a focus on improving average handover times and decreasing long waits. Improvement trajectories have been set for all the main acute hospital sites and the local NWAS team will work with their hospital partners towards achieving these.
Urgent and Emergency Care Growth
Additional non-recurrent funding was received in 24/25 to support the improvement of our response to category two patients. This allowed the deployment of additional ambulance hours across the North West. It has allowed us to add an additional 31 frontline staff (paramedics and emergency medical technicians) and deploy 400 extra hours of ambulance time per week. The majority of this additional resource was placed in Cheshire and Mersey to support demand there, but there was also extra ambulance hours added in Cumbria and Lancashire, and Greater Manchester.
The additional hours were provided to support the achievement of the interim recovery response requirement for 24/25 of a mean response time of 30 minutes to category two calls (in place of the national 18-minute mean standard), which we achieved. The funding also allowed us to provide some additional supervisory support to our frontline staff. This will help us provide clinical supervision and make sure our paramedics and emergency medical technicians are supported to provide the best care possible.
Patients we help on the telephone (hear and treat)
The ICC clinical delivery team has been working hard to improve the process of treating patients over the phone, helping reduce unnecessary ambulance dispatches. During 24/25, 15% of emergency incidents, who were initially identified as needing an ambulance, were successfully managed through triage and treated over the phone.
Positive impacts of hear and treat include:
- Reducing ambulance demand: By addressing more cases via phone, fewer ambulances are required, which can help prioritise emergency resources for patients in more urgent need.
- Improving efficiency: Streamlining the triage process helps make better use of time and resources, improving the overall efficiency of the healthcare system.
- Cost savings: Treating patients over the phone reduce operational costs associated with ambulance dispatch and A&E visits.
- Patient satisfaction: For some patients, being treated at home through phone triage can be more convenient and less disruptive, enhancing overall satisfaction with the service.
Patients not conveyed to hospital (see and treat)
As there is improvement in hear and treat rates, ambulances are only sent to the patients that cannot be helped on the phone, and these are often more complex or unwell. Some of the patients attended with a face–to face response may still be assessed by a clinician and be identified as being suitable for management by a primary care service or urgent care service, rather than needing transportation to an emergency department. This is referred to as ‘see and treat.’
Working closely with partners in heath, social care, and the third sector, pathways have been developed that provide the care required without the need for the patient to be taken to hospital. This includes access to virtual wards, response within two hours by urgent care clinicians based in the community, or specialist community pathways for frail patients, or those with specific conditions such as respiratory illness. These are just some examples of pathways that our clinicians can access to support managing patients in places other than at hospital.
In 24/25, there was a small reduction in see and treat rates, which is likely to be due to more patients being managed through assessment over the telephone and not needing a face –to face response. In 25/26, there is planning for further work with system partners to find additional appropriate ways of managing patients in the community who do not need transporting to an emergency department. This will include coordination of the care offered at place level by system partners, making it easier for an NWAS clinician to access the right solution for a patient. This will help to lessen demand on busy emergency departments and support, providing the appropriate care for patients closer to home (or in the patient’s home).
Leadership Review
Over the last 12 months a new frontline operational and clinical leadership structure has been implemented across the service delivery directorate. As well as delivering a focus on team management, supervision, and support for frontline staff, it has enhanced our response to patients. There are now a minimum of six advanced paramedic practitioners, with skills in managing critically unwell and complex patients, on duty across the region 24/7. They respond to patients that need that additional advanced skillset, such as complex maternity, acutely unwell paediatric patients, serious trauma, and cardiac arrests. There are also six duty officers, our first line operational leadership response to incidents, available across the region 24/7. They provide support at multi-patient incidents, provide our operational commander response to significant and major incidents, and welfare and wellbeing support to crews who attend difficult incidents. The changes have also seen the introduction of sector clinical leads, who work closely with the wider local management teams to improve and sustain the quality of care delivered by frontline clinicians.
The review has also increased our ability to respond to the most critically unwell patients in a timely manner, and this has already led to a small improvement in mean category one response times, with more work being undertaken to further improve these in 25/26.
Patient Transport Service
The patient transport service (PTS) contracts for Merseyside, Greater Manchester, Lancashire, and Cumbria were due to expire in 2024, however were initially extended to 31 March 2025. During 24/25, we resubmitted bids for the new contracts for the period 2025 – 2030 across three lots; Cheshire and Merseyside, Greater Manchester, and Cumbria and Lancashire and the contract was subsequently extended until 31 March 2026.
In September 2023, the PTS senior leadership team agreed a financial improvement plan to be delivered by 31 March 2025. The overarching objective was to optimise patient journeys whilst delivering financial efficiencies. Key deliverables of the plan included:
- Reducing the use of private ambulances across the service:
Through quarters one to three, the use of private ambulances reduced by over 50% per day. The result of this was a greater proportion of contracted activity delivered through NWAS resources throughout 24/25, improving the effective use of our resources.
- Recruitment of an additional 130 volunteer car drivers
Whilst the ambitious target was not achieved positively, an additional 60 volunteers were recruited with 70 more in the recruitment pipeline. Positively, the total number of volunteer car drivers increased from 128 in 23/24 to 162 in 24/25. We are extremely grateful for the invaluable service these community volunteers provide and their commitment to their communities.
Performance Activity
| Contract | 24/25 Baseline | 24/25 Activity | Activity variance | Activity variance % |
| Cumbria | 168,290 | 135,886 | -32,404 | -19% |
| Greater Manchester | 526,588 | 568,461 | 41,873 | 8% |
| Lancashire | 589,181 | 439,661 | -149,520 | -25% |
| Merseyside | 300,123 | 314,438 | 14,315 | 5% |
| NWAS | 1,584,182 | 1,458,446 | -125,736 | -8% |
Table: PTS Activity
PTS activity in 24/25 has continued to grow and is now sitting around 8% below the baseline compared to 10% below the baseline in 23/24. Although Merseyside and Greater Manchester saw an increase in activity of 5% and 8% respectively above expected levels, Lancashire experienced a reduction of 25% and Cumbria a reduction of 19% against expected activity levels. The increase in activity in Merseyside and Greater Manchester has been delivered in the context of diverse and evolving healthcare systems, with reconfiguration of hospital services, an increasing number of locations over geographically spread greater distances, with increasingly complex patients, and reducing dependence on third party providers.
It is essential to maintain an efficient and effective balance that ensures PTS meets the needs of patients, the local hospital trusts and integrated care systems, whilst delivering a high quality, responsive and financially viable service.
Utilisation
As planned in the previous year, the focus for PTS in 23/24 was to return to pre-covid utilisation of 1.8 patients transported per hour in an average eight hour shift. During the pandemic, this utilisation dropped to 1.2 due to single occupancy of our vehicles, although Covid positive patients could travel together resulting in utilisation occasionally being above 1.0.
Although the objective was to return to pre-Covid utilisation rates of 1.8, analysis has shown that since 18/19 the healthcare system has changed in relation to outpatient services. Patients are now travelling to more locations further afield, meaning that the dynamic use of resource can be challenging. Throughout 24/25, utilisation has improved and there has been an upward trend for all counties with Merseyside showing the greatest improvement at 1.51 at the end of March 2025.
PTS Improvement Programme
The Trust Management Committee commissioned a PTS improvement programme of work, which was initiated in November 2024. The improvement programme builds on the work delivered in the PTS financial improvement plan (2023- 2025)
The improvement programme is designed to improve outcomes and experience for patients and staff, whilst ensuring delivery of the contractual obligations and financial efficiencies. The work streams will deliver a modern-day logistics operation, set against the backdrop of a combination of increasing activity, increasing places of care and more stringent performance standards.
The improvement programme is an 18 month programme of work that facilitates a collaborative approach from across NWAS, with all subject matter experts to resolve some of the challenges faced by PTS, focusing on:
- Digital solutions and innovations
- Workforce and leadership development
- Improving operational productivity and efficiency
- Improving culture
- Financial efficiency as a bi product of the above
Patient Safety
Maintaining the safety of our vulnerable patients remained a priority throughout 24/25. PTS continues to trial the Furno Power Trax, tracked chair which, if successful, will enable safer movement of patients up and downstairs, whilst maintaining the safety of our staff in terms of manual handling.
We also trialled an electric vehicle, with positive feedback from patients who reported it was a much smoother and more comfortable ride. We also introduced new standard operating procedures to respond to safety legislation in the transporting of patients in wheelchairs, and played a significant part in the NWAS Flu Campaign with 97% of staff acknowledgement of the flu jab.
Digital developments
In 24/25, the text ‘NO’ to cancel service was introduced. This service made use of the three automated text messages sent to patients.
- Booking confirmation
- Three days notice
- Vehicle on route.
Patients are able to reply to the text message with a simple ‘NO’. This will result in the patients’ booking being cancelled or an abort if the vehicle had committed to collect the patient. The net result of this would be a improved patient experience through reduction in calls to cancel transport, and improvement in productivity due to a reduction in aborted journeys. Analysis of the impact of this new service is ongoing.
Development across all three service lines, PES,111 and PTS saw the introduction of a notification to the PTS service if the patient, identified by NHS Number, had made a call to 999 or 111 within the previous 24 hours. The purpose is to allow PTS dispatch to enquire if the planned PTS transport was still required. This is a new innovation and the impact is yet to be assessed but is expected to show a reduction in cancelled and aborted journeys if patients have been admitted to hospital.
Recruitment to senior management positions in the PTS leadership team will conclude, as will recruitment to PTS Team Leader roles, which will fully establish frontline supervision and provide much needed support to our staff both operationally and in terms of visibility and engagement.
Quality Standards
There are four areas of quality performance indicators within the patient transport service known as quality standards:
- Call answering
- Travel time on a vehicle
- On time arrival
- Collection after treatment
These performance indicators are based on whether the journey was planned or unplanned, or if the journey was for someone receiving enhanced priority service (EPS) including renal dialysis, or cancer treatment.
The PTS service line continues to make progress in terms of its priorities and maintaining a high quality of service to our patients and the improvement programme is designed to continue improvements against these.
| PTS Contractual Quality Indicators 24/25 | 24/25 performance |
| 75 % of calls answered within 20 seconds | 27.80% |
| Average length of time taken to answer inbound calls (Average is 60 seconds) | 04:57 |
| Planned care: 85% passenger time on vehicles is less than 60 minutes | 86.3% |
| Planned care: 90% of patients arriving within 60 minutes of scheduled appointment time | 76.7% |
| Planned care: 80% of patients collected within 60 minutes of scheduled collection time or patient readiness notification | 58.3% |
| Planned care: 90% of patients collected within 90 minutes of scheduled collection time or patient readiness notification | 79.0% |
| Unplanned care: 80% passenger time on vehicles is less than 60 minutes | 88.6% |
| Unplanned care: 80% of journeys where the patient is picked up no later than 60 minutes after booked collection time | 55.4% |
| Unplanned care: 90% of journeys where the patient is picked up no later than 90 minutes after booked collection time | 68.9% |
| Enhanced priority service: 85% passenger time on vehicles is less than 60 minutes | 91% |
| Enhanced priority service: 90% of patients arriving 45 minutes prior to scheduled appointment time | 76.0% |
| Enhanced priority service:85% of patients collected within 60 minutes of scheduled collection time or patient readiness notification | 78.7% |
| Enhanced priority service: 90% of patients collected within 90 minutes of scheduled collection time or patient readiness notification | 92.0% |
Table: PTS Contractual Quality Indicators 24/25
Commitment to recruit a PTS clinical quality lead was made in 24/25 with a focus on clinical, quality, and governance initiatives within the service, shaping and enhancing patient transport delivery, ensuring compliance with regulatory standards and driving continuous improvement across clinical operations.
Volunteers
We are immensely grateful for the support of our many volunteers who give up their free time to support us and the communities they live in. They are a vital asset to the trust, whether providing life-saving assistance in an emergency, or driving patients to out-patient appointments. We also have a significant pool of volunteers who help shape our organisation via the Patient Public Panel (PPP). These members work with us on major projects and initiatives to give a patients’ perspective and view on the decisions we make and their input is invaluable and confirms our commitment to putting the patient at the heart of all that we do.
Community Resuscitation and Engagement Teams
The Community Resuscitation and Engagement team provide leadership and training to the Community First Responders (CFRs) who support the trust. They are also responsible for working with key stakeholders and partners in the community to identify areas which require support with installation of defibrillators and/or basic life support training and education.
Community First Responders
CFRs are volunteers who are trained and activated to attend certain emergency calls where time can make the difference between life and death, such as a cardiac arrest, and breathing difficulties. They provide basic care until the ambulance arrives and can also support ambulance crews once they are on scene. Throughout 24/25 CFRs were activated to 16,295 calls.
There are two different types of CFRs volunteering in communities:
- Community First Responders (CFR) are equipped with an AED, oxygen, handheld suction, tympanic/infrared thermometer, mechanical blood pressure and wound dressings
- Enhanced Community First Responders (ECFR) have additional equipment and are trained and assessed by NWAS clinical staff to check blood glucose levels and, if required, administer dextrose gel. They are also equipped with cervical collars and CAT tourniquets. For cardiac related chest pain, they can administer 300mg aspirin. They can also administer Entonox if needed to control pain levels. Enhanced CFRs can be dispatched to a wider range of calls than the CFRs.
We have a total of 692 active CFRs split across the regional footprint as follows:
- 91 Greater Manchester
- 88 Cheshire and Merseyside
- 513 Cumbria and Lancashire
As CFR schemes are vital to support the more remote communities, there are significantly more responders in towns and villages across Cumbria.
Although work was undertaken during 24/25 to remove CFRs that were no longer active and regularly responding for the trust, the team also recruited and trained 110 new CFRs across the North West, meaning we now have more active CFRs than we had in 24/25.
In quarter four of 24/25, a new CFR training course was implemented and, moving forward all new CFRs will receive an ‘FAQ Level 3 Award for First Responders on the Scene’ qualification. It has been specifically designed for people who intend to volunteer as community first responders and the development of it was supported by the national network of ambulance service community first responder managers. The course covers the principles of ambulance service first responder care, providing knowledge and skills relating to scene safety, patient assessment, management of life-threatening emergencies, assessment and management of illnesses, medical conditions and injuries.
Heading into 25/26, the team are focussed on further increasing the number of CFRs in areas where there is a demand to supplement the core ambulance response.
Defibrillators
NWAS currently support both unlocked and locked cabinets however, in accordance with guidance issued by AACE, Resuscitation Council UK and the British Heart Foundation, the trust will be promoting unlocked cabinets moving forward. By using unlocked cabinets, this will improve accessibility to defibrillators and reduce delay in getting early defibrillation to the cardiac arrest patient. We currently have 10,000 defibrillators registered in the North West on the British Heart Foundation supported national defibrillator network known as “the Circuit”. Planning is underway for 25/26 to sustain this number of available defibrillators, and support work to increase the deployment of them to cardiac arrests.
NHS Charities Together (NHSCT)
Working closely with the NWAS Charity, our Community Resuscitation and Engagement team has accessed further funding through NHS Charities Together, the purpose of which is to aid the improvement of health inequalities and out of hospital cardiac arrest mortality rates.
The funding from NHSCT has allowed the community-based teams of engagement officers to continue to work within their local communities with stakeholders and partners to increase basic life support training, provide more life-saving defibrillator equipment, and support bringing existing community defibrillators back online.
Over the last 12 months, the team have been involved in the placement of 140 new public access defibrillators across the NWAS footprint. 25/26 will see a more targeted approach to placements of new defibrillators, focusing on areas of need, alongside reactivating defibrillators in communities that have been unavailable for some time.
As part of our winter plan, and with funding from NHSCT, the Community Resuscitation and Engagement team were able to activate volunteers to provide welfare support outside hospitals, supplying teas, coffees, soft drinks and snacks to crews who were delayed waiting to handover their patients. Volunteers attended 19 hospital sites and covered 512 hours of welfare support provision to frontline crews and were a welcome sight for our staff.
Patient Transport Service (PTS) Volunteer Car Service (VCS)
In support of PTS, a team of valuable volunteer car drivers continue to operate, making over 1.4 million patient transport journeys across the North West every year. During 24/25, there was a campaign to increase the number of volunteer car drivers to support people in the communities who need the service the most. There are currently 162 VCS drivers and in the last 12 months an additional 60 volunteer car drivers have been recruited to join the team, with a further 70 currently in the recruitment pipeline.
Resilience/EPRR
Resilience
Our Resilience team comprises of three departments, Contingency Planning, Command and Resilience Education and Special Operations, each with its own senior management lead.
Contingency Planning
Our contingency planning arrangements and capabilities assist in providing evidence of compliance with our duties under the Civil Contingencies Act (CCA), 2004, the Health and Social Care Act 2008, Regulations 2010 and the NHS England Emergency Preparedness, Resilience and Response (EPRR) Framework, together with other legislation such as the Corporate Manslaughter and Corporate Homicide Act 2007 and the Human Rights Act 1998.
The NHS needs to plan and respond to a wide range of incidents and emergencies that could affect patient care or public health. The National Risk Register (January 2025) is used to inform planning to enable us to respond to a range of emergencies while maintaining a positive response to the community as required by the Civil Contingencies Act (2004). Under the EPRR arrangements, all NHS trusts which are also designated Category 1 responders under the Civil Contingencies Act, such as ours, are required to undertake an annual self-assessment process to determine the level of compliance of resilience arrangements measured against the NHS England core standards.
Following a review of the EPRR self-assessment process in 2023, we were able to build our compliance throughout 24/25 and embed our readiness and preparedness as a Category 1 responder.
Core Standards: Out of the 58 that apply across the trust (covering PES, 111, PTS and Resilience), we have worked through the check and challenge with NHS England and submitted 52 fully compliant and six partially compliant. This translates to 90% substantially compliance. Throughout the year we continue to appraise ICB and Local Health Partnership (LHRPs) and monitor compliance through internal governance structures. This year’s compliance demonstrates the significant work carried out by the trust since 2023, improving its readiness and preparedness as a Category 1 responder.
Interoperability Standards: Out of 135 applicable standards, we have self-assessed 127 as fully compliant and eight partially compliant. This represents a compliance figure of 94% and a rating of ‘substantially complaint’. The interoperability standards are specific to ambulance trusts. Although not part of the assurance process, the ICBs and LHRPs are updated, and compliance is monitored through internal governance structures.
As part of the EPRR self-assessment all NHS trusts were required to carry out a ‘deep dive’ on a specific area to gain valuable insight. This year’s deep dive aligned to cyber security. The outcome of the deep dive is used to identify areas of good practice and further development. The Contingency Planning team lead on many exercises during the year, and one area covered an internal exercise on cyber security involving all departments across the trust.

Command and Resilience Education and Training team
In the team’s first year it has made significant progress in enhancing professional standards, training and education across command preparedness. The team has focussed on delivering training to all those involved in preparedness and response for incidents, including the executive team, all levels of command, national interagency liaison officers (NILOs), Medical Emergency Response Incident team (MERIT doctors) and commanders across the integrated care centre (ICC).
The key areas of the annual commander training covered:
- ParaFolio – National Occupational Standards (NOS)
- Communication Skills
- JDM (Joint Decision Model)
- JESIP (Joint Emergency Services Interoperability Principles)
- Interoperability – Special Operations
- Exercise scenario – strategic, tactical and operational.
- Death in service
- Flooding table top exercise and business continuity
- Debriefing and logging
The team continue to work with the People directorate to develop a training package for major incidents within mandatory training programmes for all frontline staff. The training package for all frontline staff included:
- Incident Response Plan (first on scene / windscreen report)
- METHANE sit-reps
- Ten second triage (TST) and Major Incident Triage Tool (MITT)
- JESIP (Joint Emergency Services Interoperability Principles)
The team continue to develop working in partnership with key stakeholders internally but also across the sector, specifically with other ambulance trusts in the north, and nationally with the sector lead for command and control guidance, the NHSE Emergency Capabilities Unit (ECU). Following a tendering process, the London Ambulance Service, on behalf of NHSE, lead on ECU (previously known as NARU).
One area of development relates to a digital solution for all commanders to collate evidence against their contractual national occupational standards. An app, ParaFolio, has been developed to ensure assurance is readily available for the board to ensure we are meeting our compliance standards as defined within the EPRR core standards. The app has been well received by all, and interest is growing across the UK ambulance sector.
The Command and Resilience Education and Training team are a vital resource to ensure we continue to train, educate, exercise, asses, develop all commanders and command support advisors, along with ensuring they are appraised on the latest national policies and procedures, and build their confidence and abilities when responding to any type of large-scale incident.
Special Operations
Special Operations is spread across three main disciplines. The first of which is our Hazardous Area Response Teams (HART), a 24/7 response to patients in hazardous environments such as chemical, biological, radiological, nuclear (CBRN), or hazardous material incidents (HazMat). Other responsibilities include urban search and rescue (USaR) such as collapsed structures, working at height or within confined spaces, Marauding terrorist attacks (MTA) including firearms, bladed weapons, or vehicles as a weapon; inland water incidents including swift water rescue and flooding and high consequence infectious diseases.
Our second discipline is Special Operations Response teams (SORT), paramedics and EMTs who are primarily deployed on ambulances and rapid response vehicles but who can be called upon to support our HART teams at major or complex incidents including CBRN and MTA.
The third discipline is our Medical Emergency Response Incident teams (MERIT), who are specially trained senior doctors providing advice and support at major and complex incidents.
Hazardous Area Response Teams (HART)
Following additional investment to increase the resilience and enhance the response of the HART team across the North West, recruitment was undertaken through late 2024 and early 2025 for an additional 20 paramedics to progress throughout 2025 as qualified HART members.
For the second year, we ran HART taster sessions for staff to provide an insight into what HART is and this proved to be extremely positive in terms of equality, diversity and inclusion. These taster days broke down myths and barriers for minority groups to express an interest in joining HART. The gender mix of HART staff continues to improve with a 20% increase in females joining HART. Minority ethnic groups also continue to increase as part of the Special Operations workforce.
This increase in HART establishment demonstrates our commitment to maintaining the highest standards when providing safe systems of work for staff working in hazardous environments.
Additional recruitment throughout the last year has included posts for a head of special operations, HART training manager, a group manager and administration officer.

To ensure the safety of staff when on live deployments, training is a mainstay of the HART programme. Over and above the seven weekly continuity training rota, the team has formally recertified in breathing apparatus, confined space rescue and swift water rescue, as part of the bi-annual recertification cycle. The HART team continues to grow in specific subject matter areas, increasing its instructor cadre to support internal and national training across the sector.
As reported in last year’s annual report, the trust continues to demonstrate its commitment to HART in the development of a brand new state of the art facility in the Liverpool area. The project is due to be completed in June 2025. The site will provide improved staff facilities including a gym, specialised training and education facilities, and will house the Merseyside major incident fleet.
Special Operations Response Teams (SORT)
The trust has over 250 SORT staff across the regional footprint providing an enhanced response to major and/or critical incidents, but also those that involve chemical, biological radioactive or nuclear materials and in the event of a marauding terrorist attack (MTS). SORT staff receive initial training and then refresher training throughout the year to maintain their skills. The SORT leadership team ensure the trust has approximately 34 SORT operatives on duty at any one time to enable an appropriate response to CBRN, MTA, or other similar incidents.

Additional to the training, SORT have supported several multi-agency high profile MTA, CBRN, and multi-agency exercises across the regional footprint.
The SORT team has three managers, who deliver training internal across CBRN and MTA, along with supporting command training. They also support the delivery of training and education of staff in decontamination in the acute hospital environments complying with the NHSE (NHS England) core standards requirements, improving staff safety and the quality of service to our patients.
Medical Emergency Response Incident Team (MERIT)
The Medical Emergency Response Incident team (MERIT) is intricately woven into the Quality Strategy framework, particularly emphasising safety first, highly effective care, and person-centred partnerships.
As a cornerstone of their approach, MERIT prioritises a safety-first culture by providing expert medico-legal advice to ambulance service health command structures during major, mass casualty and complex incidents. This ensures swift and accurate decision-making to protect both patients and responders. Through their meticulous training and recruitment efforts, MERIT has successfully recruited and trained four additional team members, while preparing a further five more for interviews, reinforcing their commitment to maintaining a highly skilled team capable of delivering support to the on-call ambulance service health command structure.
Led by the MERIT manager, several CPD and training sessions are held across the year covering a broad range of skill sets, and primarily relating to MERIT command roles, and the clinical casualty management. MERIT’s operational activities underscore their dedication to highly effective care, not just responding to large scale incidents but also to complex incidents supporting frontline staff with the clinical management of patients to enhance the care they require on the frontline.
This highlights MERIT’s proactive approach to continuous improvement and skill enhancement, ensuring that responders are equipped to deliver the highest standard of care in any scenario. Moreover, MERIT’s collaborative efforts extend beyond the immediate response realm, fostering person-centred partnerships through their participation in major live exercises and no-notice communication exercises. This facilitates seamless coordination and integration with other emergency response agencies for the benefit of the community they serve. MERIT is an integral part of the patient centred approach the trust takes in its role across emergency and urgent care.
Ambulance Quality Indicators (AQIs)
A key measure of the effectiveness of our services is the monthly National AQI submission to NHS England, produced by the Clinical Audit team. This is then utilised by clinical leadership teams to work with system partners to learn and share outcomes, ultimately informing local improvement workstreams.
We provide quarterly AQI reports to the Clinical and Quality Group and Quality and Performance committee. We provide further localised reporting for STEMI (ST segment elevation myocardial infarction) and the new older adult falls to our clinical leads, to contribute to learning and improvement.
Following a successful pilot during 23/24 the older adult falls AQI has been introduced to the national AQIs. Whilst NWAS sits below the national average for this AQI, there has been a significant amount of work that has gone into increasing compliance such as face to face training through the trust’s mandatory training cycle, the introduction of a falls tile within the EPR to provide structure and prompts for clinicians, whilst this has not been reflected in the performance data published to date, we know that it is positively impacting the performance and we should continue to see improvements across quarter four data and into 25/26.
Additionally, both STEMI and post ROSC care bundles have increased from last year’s data and both sit above national average. This is as a result of both changes to the trust’s EPR system for STEMI care and focused stretch targets for post ROSC care that took place towards the end of 23/24, with that data showing sustained improvements through 24/25.
The trust’s Quality Account 24/25 provides further information in relation to Ambulance Quality Indicators, together with a summary of the local clinical audits undertaken during 24/25.
Financial Review 24/25
This section outlines the financial performance of the trust for the financial year ended 31 March 2025 and the results outlined in this section relate to the full 12 months period of 1 April 2024 to 31March 2025.
A copy of the full statutory audited accounts is included in this report, together with a glossary of terms to assist the reader in interpreting the accounts.
Financial Duties Review
NHS trusts have several financial duties.
Break Even – taking one financial year with another
NHS trusts have a statutory duty to break even taking one financial year with another and we have continued to meet this duty in 24/25. NHS trusts that merge part way through a financial year, are not measured against year-on-year break even duty, as the performance summary relates to the financial performance of predecessor bodies. For North West Ambulance Service NHS Trust, measurement against the break-even duty commenced from 1 April 2007. The cumulative performance against this target for 24/25 is a surplus of £52.904m.
It should be noted that included within operating expenses in 24/25 and 23/24 are fixed asset impairments of £0.854m and £3.664m respectively. These impairments have mainly arisen because of a downturn in land and building asset values and have been confirmed by an independent valuation. The Department of Health and Social Care considers financial performance against the break-even duty to be assessed net of impairments.
Break Even – each and every year
NHS trusts have a regulatory duty to break even in each financial year. In 24/25 we returned a surplus of £6.288m and therefore achieved this regulatory duty.
External Financing Limit
NHS trusts used to have a regulatory duty not to exceed the External Financing Limit (EFL) set by the Department of Health and Social Care. From 24/25, the requirement to disclose the performance against this measure has been removed, based on this no longer being actively used in oversight by DHSC and NHS England.
Capital Resourcing Limit
NHS trusts have a regulatory duty to contain capital expenditure on an accruals basis, within an approved Capital Resource Limit (CRL). The CRL is part of the resource accounting and budgeting arrangements in the NHS and its purpose is to ensure that the resources allocated by the government for capital spending are used for capital rather than to support revenue budgets. The CRL is accruals based in contrast to the EFL which is cash based. The CRL controls the amount of capital expenditure that an NHS body may incur in the financial year.
We had a CRL of £29.851m for 24/25 and had a charge against the CRL of £29.850m – spend was in line with the resource and therefore achievement of the duty. Trusts are allowed to underspend against CRL but not overspend.
Capital Cost Absorption (CCA) Duty
NHS trusts have a duty to absorb the cost of capital at a rate of 3.5%. The financial regime of NHS trusts recognises that there is a cost associated with the maintenance of the capital value of the organisation. The trust is required to absorb the cost of capital at a rate of 3.5% of average relevant net assets. This was achieved for 24/25 and is the dividend paid on public dividend capital.
Apply the Better Payment Practice Code
This regulatory duty requires NHS trusts to pay all supplier invoices within 30 days. We achieved this duty in all categories in 24/25 and performance is summarised below:
| 1 April 2024 – 31 March 2025 | Performance |
| Non-NHS Creditors % paid within target – Numbers | 95.6% |
| Non-NHS Creditors % paid within target – Value | 97.0% |
| NHS Creditors % paid within target- Numbers | 98.0% |
| NHS Creditors % paid within target – Value | 99.4% |
Overall performance by the trust against the Better Payment Practice Code has been consistently met since we were established.
In summary, for the 24/25 financial year, we achieved all of the statutory and regulatory financial duties.
In 24/25, our total income was £554.753m where income from patient care activities was £540.410m and was generated from the following activities:
| Income from patient care activities | 2024/25 £000 |
| PES Income | 414,366 |
| PTS Income | 54,546 |
| 111 Income | 35,358 |
| Other Income | 36,140 |
| Total income from patient care activities | 540,410 |
Late Payment of Commercial Debts (Interest) Act 1998
Under this legislation, we can claim interest on the late payment of debts by contracting partners and are required to disclose amounts of interest and compensation paid during the year. During the year, we did not receive any such payments.
Financial Environment – ICS
The breakeven financial plan for NWAS in 24/25 was agreed as part of the wider Lancashire and South Cumbria ICB system deficit plan.
All parties in the system agreed a range of measures aligned to the system plan. To build a financially sustainable system for the future, with a renewed focus on cost improvement and service transformation during 24/25.
NWAS has achieved its financial duties in 24/25, although this has been challenging, particularly in the context of the current financial environment and operational pressure, whilst maintaining service quality. Our financial focus continues to be about resilience and sustainability, under ICB block contract arrangements.
Our cash balance remains strong and was £59.112m as of 31 March 2025. The trust holds its cash within the Government Banking Service (GBS).
The 24/25 capital programme for NWAS continued to invest significant capital resources to procure ambulance vehicles and equipment; enhance our digital infrastructure; investment in digital developments and to maintain and improve the quality of our estate.
Anti-Corruption and Anti-Bribery Matters
One of the basic principles of public sector organisations is the proper use of public funds. Most people who work in and use the NHS, conduct themselves in an honest and professional manner and they believe that fraud, bribery, and corruption, committed by a minority, is unacceptable as it ultimately leads to a reduction in the resources available for patient care.
We are committed to reducing the level of fraud, bribery, and corruption within the NHS to an absolute minimum and keeping it at that level, freeing up public resources for better patient care. We do not tolerate fraud, bribery or corruption and aim to eliminate all such activity as far as possible.
At our most senior level we encourage anyone having a reasonable suspicion of fraud, bribery, or corruption to report them and no employee will suffer in any way because of reporting these suspicions.
We will take all necessary steps to counter fraud, bribery and corruption in accordance with the NHS Counter Fraud standards and relevant UK legislation.
We have our own dedicated anti-fraud specialist (AFS), who is accredited by the NHSCFA and accountable to them professionally for the completion of a range of preventative anti-fraud, bribery, and corruption work, as well as for undertaking any necessary investigations. Locally, the AFS is accountable on a day –to day basis to the trust’s director of finance and reports periodically to our Audit Committee
Our People
24/25 represented the second year of the trust’s People Strategy. The strategy was refreshed to take account of the recommendations of the national Ambulance Culture report which was published in February 2024. Delivery of the strategy is supported by annual plans with oversight through the trust’s governance structure. The key areas of focus of the strategy are ensuring staff are safe, happy and healthy; that our workforce is diverse, valued and respected; our leadership is compassionate and that our people reach their potential.
Progress in ensuring our staff are safe, happy and healthy has been delivered through a number of key initiatives in 24/5. The trust was proud to have been selected to be part of the second national cohort of the People Promise Exemplar Programme. The programme funded a 12 month people promise manager who undertook focused engagement on key areas of lower performance in the staff survey, primarily engagement, recognition and flexible working, through a mix of a trust wide survey, listening sessions and attendance at management meetings. The work has now progressed to delivery programmes with area directors acting as SROs for both the flexible working and the reward and recognition workstreams.
To improve access to health and wellbeing support, the trust launched the Wellbeing Hub in March 2024 with the aim of becoming a ‘one-stop-shop’ for wellbeing related information, advice and guidance. Since its launch, the Hub has dealt with around 700 enquiries on a range of issues, providing advice, signposting or escalating where appropriate. Workforce wellbeing officers also delivered three wellbeing festivals – providing staff members with access to a range of wellbeing services, experiential activities (massages, health checks etc) and enabling them to learn more about the trust’s wellbeing offer.
Chaplain for Staff Wellbeing, Reverend Karen Jobson had a busy year with over 3,700 staff contacts. Her approach has involved offering confidential support to all NWAS staff regardless of faith and/or belief, and she has conducted over 150 one –to one sessions assisting with bereavement, family, mental health, work stress, and other concerns including support requested at major incidents. She has also provided support to teams following the bereavement of colleagues and led her first service funeral in February 2025.
The trust has also facilitated a number of additional wellbeing initiatives, including piloting a sleep fatigue recovery project. This uses smart technology to measure and improve sleep. The immensely successful and popular Beat the Burnout programme was recommissioned from Manchester Stress Institute, to provide managers in operational service lines the skills and knowledge to manage stress, sleep and healthy nutrition during the busy winter pressures. Around 85 managers took part in the four week coaching programme between Nov 2024 – March 2025, with many participants feeding back that the programme has helped revolutionise their approach to sleep and nutrition.
The major incident in Southport during the summer posed unique challenges for NWAS staff. Through the new occupational health provider, who had taken over service delivery in April 2024, the trust was able to provide a comprehensive response to support those impacted by the event. This included group decompression sessions as well as individualised support. This was supplemented through the chaplain for wellbeing who provided pastoral support during debriefs and meetings, conducted observation shifts with staff at Southport station, and offered informal support.
We managed our annual flu vaccination programme for 24/25 with a similar model as previous years. A number of clinics were set up across the region to encourage all staff to have the vaccine. In addition, flu vaccinators were deployed to offer vaccines via a roving model. We officially concluded our campaign at the end of March 2025 and the final uptake of the flu vaccine was 42.41% of staff. This position compares well with other regional providers but reflects a national trend of a low uptake of the vaccination offer.
The 2024 NHS Staff Survey found that just over half of all respondents felt the organisation takes positive action on wellbeing (improvement compared to 2023), and nearly two-thirds said their manager takes an interest in their wellbeing.
We have invested in violence prevention and reduction to help address the challenges faced by our frontline staff in delivering services. Although the team only joined the trust part way through the year, they have already started to have an impact. Their focus to date has primarily been on improving awareness and understanding of the use of body worn cameras; building relationships with police colleagues to support successful prosecutions; focusing on the experience of hate crime and verbal abuse in our contact centres, including addressing frequent abusive callers and through an improvement project helping to reduce incidents of physical harm to staff.
Equality, Diversity and Inclusion
Ensuring our staff are diverse, valued and respected has continued to be at forefront of the trust’s approach – both, in terms of workforce and service delivery. In 24/25, we refreshed our EDI Priorities which were agreed by the board in July, and are now in place until 2027:
- Priority one: We will embed fair and inclusive recruitment and progression processes to improve the diversity of the workforce at all levels.
- Priority two: We will educate and empower our workforce and leaders to promote a positive psychologically safe culture, to support a reduction in the experience of bullying, harassment, discrimination and an improvement in retention.
- Priority three: We will reduce health inequalities for our patients.
Progress against each of the EDI priorities continues to be monitored through a formal group led by the deputy chief executive, with oversight through both Trust Management Committee and board.
Key initiatives to promote inclusion and help meet our public sector equality duty have included the introduction of a new Equality, Diversity and Inclusion Statement and an Anti-racism Statement. The EDI Statement has been developed to replace the EDI Policy, as the latter reached its term limit in summer 2024. The Anti-racism Statement was developed to set out in clear terms the trust’s commitment to becoming an ‘anti-racist organisation’.
We have continued our positive action work to focus on improving representation of currently underrepresented groups within the workforce. In the last year, we participated in over 30 careers events across the North West and delivered 15 bespoke careers sessions – aimed at engagement with black and minority ethnic (BME) communities. Over 40 applicants received personalised one–to one application/interview mentoring support, and around 50% of these were successful in securing a role in the trust. Overall, we have improved our representation of BME staff by 0.7%, exceeding its target.
A significant campaign during 24/25 was undertaken, to improve sexual safety of staff and learners. The campaign launched with a clear statement setting out our expectations and this was supported by a range of additional guidance and a focus on improving reporting. We hosted roadshows to discuss the campaign with staff and a range of interventions to support managers to address issues in the workplace, including five culture events. A Civility Saves Lives session was introduced for all new staff joining the trust and as part of management inductions, setting out our expectations of behaviour in the workplace, including sexual safety. Bespoke work has also been done alongside our higher education partners to support learners to raise concerns. The NHS Staff Survey indicates a 5% increase in reporting of bullying and harassment as a result of the campaign.
At NWAS, we see diversity as a strength, and we celebrate difference. For this reason, we proudly continue to facilitate five staff networks – each empowered with their own budget and supported by an executive sponsor. The Armed Forces, Disability, LGBT+, Race Equality and Women’s Networks are part of the fabric of our trust, and each plays a vital role in helping create an environment where staff can feel comfortable in bringing their whole selves to work, to deliver inclusive and patient-centred care.
Examples of the work undertaken by our networks include a celebration event for Armed Forces week in June 2024, involving a British Army medical regiment led by a serving NWAS paramedic who is also a sergeant major. The regiment showcased their medical equipment, shared insights into the challenges of being a combat medical technician and talked to NWAS colleagues about career opportunities as an Army reservist.
The Disability Network collaborated with the Communications team to film various colleagues highlighting the significance of reasonable adjustments. This initiative was unveiled at the Network’s third anniversary celebration event, themed ‘Disability Livelihood and Employment’ which included a ‘reasonable adjustments station’, where network members showcased specialised equipment used in their roles.
During LGBT+ History Month in February 2025, the LGBT+ Network members shared testimonials about inspiring figures in LGBT+ healthcare, like Dr. Michael Farquhar who created the NHS rainbow badge for LGBT+ service users. The Network also organised a visit to Manchester’s People’s History Museum, where attendees explored the newly opened LGBT+ archives in celebration of LGBT+ History Month.
The Race Equality Network has continued to engage in supporting improvements to our recruitment practices. Members have learned from conferences like the Asian Professionals National Alliance and shared best practices and insights on international recruitment and onboarding for better retention rates. The network also supported the ParaMedic residential programme (delivered as a partnership between NWAS and College of Paramedics) at Edgehill University in August 2024. Members shared their career experiences with a group of young people from ethnic minority backgrounds who were interested in healthcare careers.
The Women’s Network has continued to grow considerably in membership and scope over the last year, with nearly 250 members as of March 2025. The Network’s main focus remains on improving maternity experiences by researching within the organisation, collaborating with HR to improve internal policies, and working with the national ambulance sector workstream to improve maternity processes and policies.
The trust has met all its statutory and regulatory reporting requirements in relation to Equality, Diversion and Inclusion, publishing its Workforce Race Equality Standard, Workforce Disability Standard, Gender Pay Gap and Equality Delivery System data. All saw improvements in a number of areas.
We were also pleased to be re-accredited as a Disability Confident Leader (Level 3) by the Department for Work and Pensions for another three years, demonstrating our commitment to an inclusive work environment for disabled colleagues.
For the third consecutive year, we have achieved the Gold Standard in the Employers’ Network for Equality & Inclusion’s (enei) Talent Inclusion and Diversity Evaluation (TiDE) accreditation. We were one of only 25 Gold Standard winners out of 185 global entries, from across 26 different sectors. With an overall score of 94%, we were the third highest ranked organisation out of all entries this year.
In February 2025, we were also re-awarded Veteran Aware status following the one-year review. We were recognised as being exemplars of the best care for, and support to, the armed forces community; and in demonstrating our commitment to the Armed Forces Covenant.
Workforce Development
In order to ensure our leadership is compassionate, NWAS’ foundation leadership programme Making a Difference has been refreshed. The programme includes modules on Leadership of Self, Leadership of Others, Leading Change and new Leading for Diversity and Inclusion and Civility Saves Lives modules. A Leading People through Systems module is in development. Leadership of Others has been delivered to 386 leaders, Leadership of Self to 357, Leading Through Change to 180 and our new Leadership for Diversity Inclusion module has been delivered to 55 leaders.
We continue to offer Chartered Management Institute (CMI) courses and refreshed the offer to include:
- Level 3 Award in Principles of Management & Leadership with 13 staff completing this year.
- Level 5 Certificate in Management & Leadership. 15 learners have commenced this course this year.
- The new Level 5 Certificate in Professional Coaching Practice. 6 learners have commenced this course this year.
A new leadership induction was delivered to over 400 leaders in the PES service line, following the implementation of the refreshed leadership roles. The Civility Saves Lives module was delivered within this.
Large scale leadership recruitment exercises took place aligned to the revised PES leadership roles. Due to scale, there was an opportunity to deliver this on a regional level and the new appointments saw an increase in female leaders in the PES service line. The refreshed process now includes appropriate assessment of commander competencies required as part of the new leadership roles.
A talent management programme to support aspirant leaders has been developed and approved, which will support up to 50 aspiring leaders across all NWAS functions.
Over 400 trust leaders have attended a one day culture event which included support sessions focussing on sexual safety and impact on NWAS staff, allyship and generational differences.
We continue to offer areverse mentoringprogramme which provides senior leaders with the opportunity to be mentored by a member of staff with very different lived experiences. The first programme concluded with a celebration event in April 2024 and the second programme launched in September 2024 with 17 reverse mentoring pairs. Practical examples of the benefits of the programme have already been shared where changes have been made based on the learning from the programme.
We also aim to ensure that our people reach their potentialand, in order to achieve this, we have continued to focus on a range of supportive measures during 24/25.
We have revised and refreshed the approach to induction and onboarding, developing NWAS, team and local induction approaches. Since October 2024, senior leaders have delivered an NWAS Welcome presentation– reaching over 700 new starters.
More than 40 different workshops and learning opportunities are offered to leaders and staff, supporting personal, team and organisational development, underpinned by strategic objectives. This year 3,394 members of staff have accessed learning and development workshops. We have introduced application, interview and assessment centre workshops this year with 364 people accessing these to prepare for career moves across the organisation.
We have delivered 11 workshops to support our neurodiverse staff, with 351 attendees. An additional 96 have completed the online learning module. We have referred two staff for our neurodiversity screenings, and eight staff for neurodiversity workplace needs assessments.
We internally produce technology-enabled learning (TEL) to support staff in their development. In total, 197 hours of video have been watched by staff. The team produced digital materials for culture and leadership events, saving an estimated 18,225 pieces of paper that would have been printed.
The CPD and Learning Hub provides staff with easier access to CPD opportunities. In 24/25, the online hub had 77,798 visits from 31,829 user sessions. There are 302 active pages of resources and information, with 331 events displayed for the next 12 months. Rapid Recap resources have received 11,209 page visits, and maternity resources have received 2,818 visits.
We support access to higher education study for clinical staff as part of the continuing professional development (CPD) offer with 675 modules supported. Working with a local university provider we have developed skills based CPD sessions delivered across the NWAS footprint, with 192 attendances.
The trust also supports the continued professional development of staff across a spectrum of disciplines, responsive to learning needs identified through the appraisal process and personal development plans. 144 external courses were supported including 39 at level five and above were supported ranging from attendance at single day workshops to supporting Masters degrees.
The EMT1 bridging programme supports staff to gain the Level 4 Diploma Associate Ambulance Practitioner qualification, which supports long-standing EMTs to develop and access the paramedic apprenticeship. 426 EMT1s have now achieved the qualification with an additional 16 currently on the programme.
We have maintained an Aspirant Apprentice EMT Programme, recognising and supporting internal talent. We currently have 56 people that are being supported through the process. Since the start of this programme in 2021, we have supported 116 members of staff to successfully transition into EMT roles and 11 into Urgent Care Services roles.
We offer open access to maths and English qualifications to all our staff, with 120 registrations on programmes.
The trust continues to deliver and grow apprenticeships across the workforce and through 24/25, we saw 327 employees registered on apprenticeships in various roles and 195 completions .
Against the Department for Education apprenticeship monitoring for public sector organisations, our position for 24/25 is set out below:
| Percentage of apprenticeship starts (both new hires and existing employees who started an apprenticeship) as a proportion of employment starts between 1 April 2024 to 31 March 2025 | 32.9% |
| Percentage of total headcount that were apprentices on 31 March 2025 | 9.6% |
| Percentage of apprenticeship starts (both new hires and existing employees who started an apprenticeship) between 1 April 2024 to 31 March 2025 as a proportion of total headcount on last day of previous period | 4.4% |
Apprenticeships underpin our approach to workforce growth and development with:
- New emergency medical technicians (EMT) undertaking a Level 4 apprenticeship
- Up to 120 EMTs able to commence on a paramedic apprenticeship, whilst remaining in employment
- Advanced clinicians supported through higher level apprenticeship study the L7 Advanced Clinical Practitioner Apprenticeship
- A wide range of corporate and support functions using apprenticeships to support existing and new staff, in areas such as finance, fleet, communications, public health,
In 2024, NWAS ranked 21 in the Department for Education’s Top 100 Apprentice Employers. We were also awarded Apprentice Employer of the year in the Lancashire and South Cumbria ICB apprenticeship awards.
All staff new to patient contact roles (including those through internal promotions) will complete an induction programme delivering the required knowledge, skills and behaviours required for the roles.
- 203 emergency medical technicians (EMT) – Level 4 Associate Ambulance Practice apprenticeship which NWAS delivers as an employer provider.
- 347 call handlers, across a range of levels
- 213 newly qualified paramedics
- 13 urgent care assistants
- 123 patient transport care assistants
As a trust, we also undertake a range of activities supporting our learners and future workforce. We hosted 246 direct entry students on a full day’s induction across the three areas of the trust to prepare the students for their practice placement time, ensure their safety and for them to have the best learning experience over their three or four years with NWAS. A number of topics were covered which focused on wider trust priorities, for example: sexual safety, Freedom to Speak up and professional standards. The induction days proved to be an invaluable foundation for students embarking on their new challenging yet rewarding career. Both colleagues and students gave positive feedback, commenting on the opportunities to interact with each other in an informative and relaxed atmosphere.
The Widening Access team has supported over 125 internal and external staff career progression with next steps information advice and guidance, application support, interview technique and confidence boosting. We have run online support sessions or a variety of NWAS roles reaching over 700 candidates. Five pre-employment programmes have also been delivered supporting 23 people into employment and our cadet programme has been successfully delivered to 46 aspirant healthcare students. To further our reach to the future workforce, we have piloted the use of live chat. This enables access to careers information advice and guidance for colleges and schools and the offer of support will be extended to 65 colleges and sixth forms across the region in 2025.
NWAS co-delivered a three day ‘ParaMEdic experience summer school with the College of Paramedics, Edge Hill University and St John Ambulance for young people aged 16 to 26 from ethnic minority groups. 42 young people from ethnic groups (recruited from St John Ambulance cadet schemes) attended the programme from 13 – 15 August 2024. They spent time in university and NWAS and were introduced to clinical skills, call taking and the HART team. The final day provided additional support around ambulance careers.
We exceeded our target for completions ofappraisals. For NWAS as a whole, by the end of March 2025, the trust position was 86.08% of our people with an up –to date appraisal with their manager against a target of 85%. We also launched an online version of the appraisal, providing more flexibility for completion.
Statutory and mandatory training delivery is a mix of face to face and e-learning for our paramedic emergency services (PES) and PTS staff, with other staff groups using e-learning . The overall 24/25 year end position is 91.17% compliance against a target of 85% and with all operational service lines exceeding the 85% target.
The core of the annual delivery is the NHS Core Skills Training Framework (CSTF) which sets out the approach to statutory and mandatory topics for NHS trusts in England. CSTF subjects are delivered across a mix of face –to face classroom days and e-learning modules, depending upon the staff group. In addition to the CSTF requirements, we prioritised the following additional subjects in the 24/25 statutory and mandatory programmes. These were determined through collaboration across multi-disciplinary subject matter experts and were informed by incident and risk:
- National level two patient safety syllabus e-learning mandated for all patient contact staff. The level one module was mandated for all non-clinical staff.
- Zero suicide alliance module
- Ambulance specific dementia tier 1 e-learning module (all staff)
- Ambulance vehicle fires e-learning module (all staff)
- Falls assessment (PES)
- Pocket mask (PTS)
- Maternity and newborn care (PES)
- ACS – STEMI (PES)
- An annual medicines management update was delivered to all relevant clinical staff in line with updates to patient group directive (PES).
NHS England is leading work to optimise, rationalise and redesign statutory and mandatory training to improve staff experience, deliver better outcomes and reduce the time burden. The NHSE StatMand programme sets out key deliverables for each NHS trust and NWAS has met all milestones set for delivery in 24/25.
In addition to the regular review of a range of workforce indicators, we use the annual NHS Staff Surveyas a key indicator of progress in deliveringimprovements in staff experience.
In 2024, over 3,550 NWAS staff participated in this, which equated to a 48% response rate. This was the highest ever number of responses we have received. The median response rate in the ambulance sector was 49% this year.
The NHS Staff Survey continues to be aligned to the NHS People Promise, and our 2024 results show stabilisation of the People Promise scores, and improvements for some of the themes.
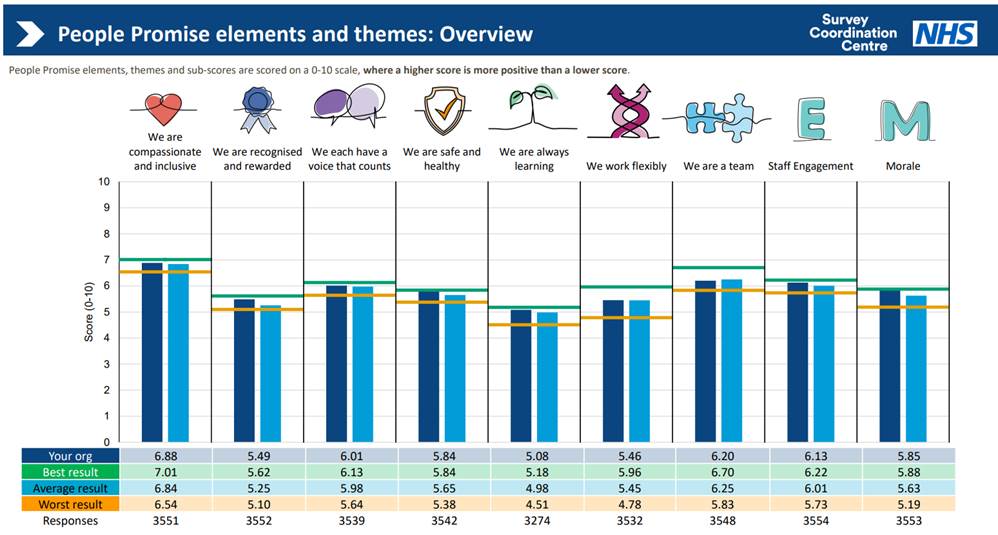
Improvements in the ‘We work Flexibly’ and ‘Morale’ themes were identified as significant. We have the best result in the ambulance sector for ‘We are Safe and Healthy’.
Other notable improvements in responses include:
- In 2024, 46% of respondents said there were ‘enough staff at organisation to do my job properly’, which is a substantial increase compared to 2023, and significantly better than ambulance sector average (35%).
- For the first time, more than 40% of respondents said they were satisfied with flexible working opportunities.
- Around half of the organisation continues to have confidence that the ‘organisation acts fairly in respect of career progression’. A 5.5% increase in positive responses can be seen from BME staff (Workforce Race Equality Standard metric) in 2024 from 2023.
- 71% of respondents who identified as disabled/having a long-term condition indicated reasonable adjustments had been made for them, and this is an improvement on 65% in 2023.
Detailed results have been shared with the board as well as directorates and teams across the organisation and are being used to inform and influence positive change to improve staff experiences.
Communications and Engagement
The Communications and Engagement team is the voice of the organisation, working alongside operational and corporate colleagues to support staff and managers, as well as providing information, news and advice to the public and our stakeholders.
The team, which is divided into two sub teams – Communications and Patient Engagement, consists of professionals with a wide range of skills including media handling, internal communications, stakeholder and patient engagement, social media, campaign planning and filming. The team also supports our very successful Patient Public Panel scheme and engagement with various patient groups within the communities we serve.
We launched our new Communications and Engagement Strategic Plan for 2024-2027 this year and this is supported by an action plan which sets out the objectives of the team on a 12 monthly basis. The plan adapts to influences from outside of the trust, supports our Trust Strategy and is created using contributions from the wider team.
The team places patients at the heart of the organisation and supports the delivery of care for our communities through the timely and accurate flow of information to the region’s diverse communities, as well as engaging with stakeholders, partner organisation and our own colleagues.
Communications
The Communications team are specialised professionals with vast experience of hosting creative, award winning PR campaigns, crisis communications, social media management, major incident handling, press relations, web management, events and staff, stakeholder and political engagement.
Their knowledge and experience enables them to be able to respond quickly in the event of urgent media enquiries or issuing information to staff and managing our response in the event of high profile incidents.
Southport 29 July 2024
Incidents which receive national and international attention are thankfully uncommon but when they do the Communications team have to think quickly and ensure information released to the public is accurate and prompt. This is supported by a well-rehearsed Communications Incident Protocol which is regularly reviewed based on the lessons learnt from each significant incident.
For events such as the tragic, fatal stabbing of three little girls in Southport in July, the media spotlight is unwavering and it is important that we work closely with our blue light colleagues and other NHS trusts to ensure consistent messaging.
Supporting the trust and our staff and engaging with the community does not end once an incident of this scale is over. In the subsequent weeks, we were extremely honoured to support the visit of His Majesty King Charles III to Southport Fire and Ambulance Station. The King met a number of staff who had been involved on the day from both the frontline and behind the scenes.
Later in the year, the Communications team facilitated a meeting of staff with the Prince and Princess of Wales. In January 2025, the government announced a public inquiry into the events of that day and we will be fully co-operating with this when the time comes.
Our thoughts are with the victims and the families.
Have we got news for you?
As one of the largest and busiest ambulance trusts in the country, the activities of our organisation is of significant interest, both nationally and locally.
In 24/25, we handled more than 600 media enquiries and issued 69reactive statements and 96 proactive press releases. In addition, we were able to secure 31 television and radio opportunities both nationally and within the North West.
We also worked with the media on a number of planned articles and features, most notably, our work with the BBC regarding violence and aggression against our staff. As part of our winter plan, this subject is an emotive one and, as we see figures rise during the pre Christmas ‘party’ season, we identified case studies which featured in a number of regional and national TV news programmes. The BBC joined us on a night shift in Blackpool and in our call centre in Greater Manchester to talk directly to staff about their experiences. We worked with the trust’s new head of violence prevention, reduction and security, to drive home the message that we will always push for prosecution if our staff are physically or verbally assaulted and this work will continue into 25/26.
We love to tell great stories about our staff and our patients and none reflect the amazing work our frontline colleagues do more than a patient reunion. We get many requests for patients to meet with the staff who saved their lives and some of these make their way into the news generating great responses from the public.
In November, we told the story of Valerie West from Whitehaven who suffered a cardiac arrest while out walking in the town and in September, we reunited Chris Jamieson from Blackpool who had a heart attack on the promenade. The media also featured the delightful meeting of baby Maeve with the call handler who talked mum through the birth over the telephone when Maeve decided to make a surprise appearance early.
Quite rightly, on behalf of their audiences, the media also hold us to account and we know there are times when we have to answer to their questions when we haven’t done so well.
We pride ourselves on answering those questions factually and with empathy, ensuring the public have the whole story and a clear understanding of our position and challenges. We do not shy away from difficult questions, we answer with honesty, clarity and openness and work with senior managers to provide the information that the public are entitled to.
The world of social media
Like it or loathe it, social media is here to stay and plays a crucial role in how we engage with our communities.
Its use is invaluable in being able to quickly publish important warning and informing information in the event of a major incident, to act as a news source for journalists and of course, for us to showcase the great work our staff do.
The trust has an official presence on Facebook, X (formerly known as Twitter), Instagram, You Tube and Linked In.
The team plans engaging posts with clear messaging about our service, the current pressures and demands, supporting our campaigns, recruitment, public health information and engaging stories about our people and the work they do.
Facebook is our most popular social media site with 93,951 followers, X comes a close second with 68,580.
Overall this year we have published more than 2,000 posts across our social media channels, which also includes Instagram, LinkedIn and Threads which have garnered over 1.3 million engagements.
The team carefully monitors activity and engagement on the sites, continually learning about what type of posts have a greater reach and impact, which, in an ever changing social media world, can be a challenge.
We strive to use striking visuals, including films made by team members as these do seem to hugely improve our reach. The shocking video which featured a real life recording of a 999 caller abusing our staff hit 276k views and was picked up and featured in the media as part of our winter campaign. Likewise, a fun video in which two crew mates gave Halloween safety advice had 298K views.
Posts are planned to coincide with known periods of high operational demand to support our frontline teams, and to give out urgent warnings of issues such as severe weather and demands on service.
Inside Knowledge
The team also runs a closed Facebook group to engage with staff and currently has 2.8k members. The group enables two-way engagement as staff can respond and comment on posts and any enquiries are forwarded to the relevant department for an informed response. Posts are published by the Communications team but staff can also post queries, their own photos and news, and reach out to each other for events, collaboration etc.
The group has been a great asset since its conception during the global pandemic and helps to reach our staff on a platform they choose to use personally. With a predominately mobile workforce, we are constantly reviewing new ways to reach and engage with colleagues.
Towards the end of 24/25, we launched a trust wide audit of the internal communications provision within the trust. This is ongoing at the time of publication and the findings will be used to identify where improvements are required and to gain a better understanding of how staff want to receive information from us. The audit is being conducted via an online survey, as well as face to face discussions with teams.
The team communicates with staff using a number of methods, with email being the most widely used and accessed. Most email bulletins are issued via ‘E-shot’ which enables reporting of who opens the communications and when. This helps us identify what information staff are particularly interested in and any pockets of disengaged colleagues.
As the workforce is predominantly operational, we issue subject specific stand alone bulletins on clinical and operational subjects to ensure frontline staff are up to date with issues relevant to them. Bulletins have also been issued on subjects such as filming of staff by patients, cyber security, pay uplifts, pensions and project updates.
To support the trust’s wellbeing offer, we issue the monthly ‘Better Health, Better You’ newsletter which contains health and wellbeing information and personal stories that staff are willing to share with colleagues, such as caring for someone with dementia, cancer survival and parenting neurodivergent children.
Each week, the team publishes a message from the chief executive and a news bulletin with stories linking back to the trust’s intranet site, aptly named the ‘Green Room’. As part of the ongoing internal communications audit, all of these methods will be examined and reviewed in the coming year.
Our staff are amazing and they do amazing things! We are firm believers in recognition and the team supports ‘shout outs’ to colleagues via the staff Facebook group and supports the annual Long Service awards which take place in each area for staff serving 20 years or more. We also run a virtual peer to peer card scheme where colleagues can send praise, express thanks, say happy birthday or let someone know they are ‘thinking of you’. In the past year, over 1,300 colleagues have received a card through the scheme.
The highlight of the year, is the annual Star Awards, a glittering evening fully funded by sponsorship and the North West Ambulance Charity, which recognises staff nominated by their peers in a range of categories.
This years’ event took place on 28 March at Ribby Hall Village in Preston and was hosted by comedian Phil Walker.
The Star Awards is a fantastic opportunity for us to celebrate achievements, whether that is for going the extra mile, supporting our communities, achieving something outstanding or being simply seen as a brilliant role model. More than 270 nominations were received in categories such as Apprentice of the Year, Inspirational Role Model and Community Contribution and a great night was had by all.
Project Support
Communications is an integral part of any project within the organisation and a great deal of work goes on to support a variety of initiatives. The team actively encourages anyone undertaking a project to consider the stakeholder impact and involvement, and the expertise of our team is well placed to act as advisors and undertake these actions.
Whether the audience is external or internal, we identify the objectives and timescales and then produce a clear communications plan which then forms part of the project’s overall strategy.
A project we support each year is the NHS National Staff Survey which is one of the largest workforce surveys in the world and is carried out to improve staff experiences across the NHS. Over the years, take up amongst staff has been low but using incentives and a more innovative and creative approach, such as targeted management messaging, and promoting the role of the people promise manager, we were pleased to see our largest return yet in 24/25.
Promoting a healthy, safe working environment has also been a priority this year and the team supported the sexual safety project with a roadshow and articles to encourage staff to either report incidents or share experiences. This work linked directly into a campaign undertaken by the Association of Ambulance Chief Executive’s (AACE) and the NHS national survey.
The team also played a pivotal role in the operational leadership review with regular bulletins, films, dedicated intranet pages, updates on the new staff structure and supporting recruitment sessions.
Other internal projects which the team supported include the flu vaccination campaign, the creation and promotion of ‘five minute’ briefings to cover multiple topics ahead of any CQC visit, the sexual safety roadshow, and the right care steering group and its work on call before convey initiatives.
Our team are also part of major estates project teams, the most significant currently being that of the new HART base in Liverpool – a £14.5m investment on the site of the trust’s former Cheshire and Merseyside Area Office.
To create a community element to the project, we partnered with two local schools and facilitated site visits, the burying of time capsules and educational sessions which will culminate in the unveiling of children’s artwork in the building when it opens in the summer of 2025.
The year has seen considerable support to the trust’s Resilience team in terms of training for commanders and senior operational leads on the importance of communicating to staff and the public in the event of a major incident. This work continues into 2025 with a focus on crisis media training.
A review of our Communications Incident Protocol was undertaken in line with the requirements set out by NHS England and a log established to ensure all Communications colleagues with press on call duties attend major incident exercises on at least one occasion per year.
Campaigns
The team’s most significant public campaign is the annual winter plan which is designed to help our operational colleagues during their busiest time of the year. It’s objective is to reduce the number of unnecessary or low acuity call numbers, manage the expectations of the public and provide health advice for minor ailments.
The actions are designed to support in the region wide objective of alleviating pressure on the wider healthcare system and we work closely with the Integrated Care Boards (ICBs), NHS England and acute trusts to align our campaigns to achieve this.
Each year, specific topics are selected based on activity for the previous winter – this year we focused on repeat prescriptions, one of the highest reasons for calling the 111 service, self-help and falls prevention, with falls being one of the most common reasons for calling 999.
Using social media, films, press releases, focus groups and visits to communities, we co-ordinated a four month long campaign tacking these subjects and as this report was being published, the results are being evaluated in preparation for next year.
Freedom of Information
The trust’s compliance with the Freedom of Information (FOI) Act 2000 falls under the Communication and Patient Engagement team’s remit, and this year, we received more requests than we ever have before.
In order to educate those we need to provide us with the data being asked for, the trust’s FOI officer undertook a training programme to highlight our legal obligation to comply with the FOI Act. This was delivered to more than 16 teams throughout NWAS and will be refreshed and continue next year.
To support the delivery of our FOI obligations, the team updated its FOI and Environmental Regulations policy in 24/25 and this is now available on our intranet site.
We are pleased to report that we ended the year with a 99 per cent compliance rate against an internal target of 95 per cent and the Information Commissioner’s Office (ICO) legal target of 90 per cent. This is despite seeing a 14 per cent increase in requests with 500 received this year.
Subjects vary but there are common themes such as activity, performance, violence against staff, vehicle numbers and drug policies, with many requests coming from the media and public figures.
Of all these requests, only one has been referred to the ICO in response to an exemption being applied. As yet, the outcome of this is unknown.
This year, we were also subject to a ‘spot check’ audit by the ICO who asked for data relating to our FOIs, overdue requests and extensions, the application of exemptions, internal reviews and compliance for quarter three (Oct-Dec 2024). No further feedback was received following our compliance with this request.
Stakeholders
Covering the whole of the North West of England, the trust has a considerable number of stakeholders who have a vested interest in the activities of the trust.
The Communications team has a role in engaging with these and ensuring they have up to date information on the subjects they are interested in.
All MP general correspondence is co-ordinated by the team and in 24/25, 13 response letters were issued on topics such as how we triage callers, medical flags on addresses and access to locations. In addition, we facilitate visits by MPs and council members to our sites. This year, we welcomed Health Minister, Wes Streeting MP to meet those involved in the Southport incident and Chris Webb MP who met staff at Blackpool station.
In addition, the Communications team co-ordinated attendance at seven council overview and scrutiny committees, supporting local managers with presentations and reports.
Regular updates are issued via a quarterly Stakeholder Briefing with ad hoc editions being sent should there be significant news, such as the announcement this year of our new chief executive.
On occasion, the trust is asked to provide a response to the Department of Health in preparation for a submitted question to be asked in the Houses of Parliament. This year, we received two such requests on the subjects of employees changing their station base and ambulances displaying Pride colours.
Web/Green Room
Between April 24 and March 25, we have had 1,196,948 engaged sessions on our website, an increase of 29.6% – this is a particularly large increase compared to other years. While there were significant spikes in page views when certain job vacancies were announced (particularly call handler roles), this increase is largely down to the ‘Southport major incident’ news page we created and directed people to on Monday 29July.
As with previous years, the most visited pages throughout the year are vacancies, apprenticeships, PTS section and our locations. Work has continued in maintaining an accessible site that meets WCAG 2.2 standards.
In Q4, a review of Ambulance Academy – the area of the site dedicated to children and young people – began in order to establish where improvements could be made to the users’ journey and where content could be developed to ensure user experience and satisfaction. This new work will be ready to go live in quarter one of 25/26 with the aim of increasing engaged sessions even further.
The Green Room is the trust’s intranet site which is available to all staff via laptops, mobile phones, and iPads. It contains a wealth of information including news, policies, guides, learning and various reporting forms.
In 24/25, we have had 1,321,620 page views on the Green Room – not including home page visits which is the default landing page on desktops. During this period, there have been more than 223,000 library files opened or downloaded, including policies, procedures and bulletins, which suggests that it continues to be a useful way for staff to find information.
As with previous years, the most visited pages include the managers on duty area, the HR portal, bulletins, and the library section. Feedback on user experience continues to be sought, including in the recent internal communications audit, in order to help shape the future of the Green Room and how we develop it to be the key source of information for all staff.
Filming
We are very lucky to have a skilled videographer within the team who works to provide the entertaining and informative videos seen on our social media sites, training videos and internal engagement films to staff.
As the demand for this service has increased, the whole Communications and Patient Engagement team enjoyed a two day training session on film making and editing, which has expanded our ability to use film rather than the written word for a substantial proportion of our communications. This is particularly useful for both our internal and external social media sites and makes for more engaging and personal engagement between senior managers and staff.
Films made this year include those to support trust projects such as sexual safety, the leadership review, hospital handovers and patient safety learning. In addition, our videographer presents a staff or patient story in each board meeting via a short film with a focus on learning and improving.
Next Year
While much of the team’s work is reactive, there is much planning done at the start of each year to set communication and engagement objectives.
As mentioned earlier, we will be looking at the results of our internal communications audit and identifying how we can improve this from both an effectiveness and capability perspective. As part of this, we will embed new methods of listening to ensure staff voice and feedback is at the heart of communications.
We will relaunch the colleague card scheme to recognise its expansion of different card types. We will also be reviewing our intranet site the Green Room as with new software and technology now available to us, we know that this can be improved to make it more user friendly.
To further embed accessible and inclusive communications across the trust, we will refresh our brand, ensuring the contrast in our colour palette is of the required standard, and continue to make accessibility everyone’s business, through promotion of the standards required to be fully inclusive and by creating an online accessibility training module for colleagues.
We intend to review our media handling protocol and continue to conduct regular reviews of our Communications Incident Protocol taking into account learning from incidents.
Patient engagement and experience
Each year the trust’s Patient Engagement team deliver an extensive patient engagement programme in line with our Patient Public and Community Engagement Implementation Plan. The plan sets out the ways we propose to engage with and obtain feedback from our patients across all service areas, including our paramedic emergency service (PES), patient transport service (PTS), the NHS 111 service and our urgent care desk. The plan also supports the trust Quality Strategy aims of ‘person-centred partnerships’ with our patients, public and communities.
A minimum 1% of PTS and PES see and treat patients are offered the opportunity to provide Friends and Family Test (FFT) feedback monthly via SMS text channel, and each week a random 300 NHS 111 patients receive the nationally mandated NHS 111 patient experience postal survey. We now offer predominantly digital opportunities to provide feedback using SMS text invites to deliver digital links to our online surveys. We also continue to review our Quick Response (QR) code feedback posters and returnable postcards on both 999 and PTS ambulances for patients to be able to provide real time feedback.
We have used a combination of virtual and face –to face engagement methods to engage with specialist community patient groups depending on their preference. We have been able to listen to the issues and experiences of our patients from mixed diverse and ethnic communities at our five Ambulance Awareness events, university freshers’ fayres and other large footfall events across our footprint.
Patient experience surveys and the Friends and Family Test 2024-2025
We provide tailored surveys across our 999, Urgent Care, PTS and NHS 111 services, inviting patients and carers to share their experiences. These are reviewed annually by service teams and our Patient Public Panel (PPP) to ensure they remain relevant.
The FFT asks whether patients would recommend our services and allows them to explain their views, offering valuable insights that are vital in transforming our services and improving patient experience.
In 24/25, we received over 25,588 responses, with a return rate of 7.54% – a 1.33% decrease from the previous year. The NHS 111 postal survey saw the highest return rate at 10.29%, reflecting strong ongoing engagement across feedback channels.
| Patient Engagement Survey – Survey Channels (April 2024 – March 2025) | Completed Returns | % of Total | |
| Patient Transport Service Patient Experience Survey | Via SMS delivery – On-line completion | 1,392 | 5.44% |
| Patient Transport Service FFT | SMS Text completion | 13,545 | 52.93% |
| Patient Transport Service FFT | Post cards | 541 | 2.11% |
| Paramedic Emergency Service Patient Experience Survey | Via SMS delivery – On-line completion | 912 | 3.56% |
| Paramedic Emergency Service FFT (See and Treat). | SMS Text completion | 6,589 | 25.75% |
| Paramedic Emergency Service FFT (See and Treat). | Post cards | 47 | 0.18% |
| Paramedic Emergency Service FFT (Comment Card) (Conveyed patients). | Post cards | 287 | 1.12% |
| Urgent Care Service Patient Experience Survey. | Via SMS delivery – On-line completion | 482 | 1.88% |
| National NHS 111 Service Patient Experience Survey | Postal | 1,553 | 6.07% |
| Localised NWAS NHS 111 Service \Patient Experience Survey | Via SMS delivery – On-line completion | 240 | 0.94% |
| Total | 25,588 | ||
Table: 24/25 Patient survey channel (data as of 18 March 2025)
Feedback received during 24/25 shows high regard for ambulance services and particularly the care and treatment provided by staff. A high 93.4 % of PTS and 90.6% of PES patients respectively stating that they were ‘cared for appropriately with dignity, respect, kindness and compassion’.
| Patient Engagement Surveys SMS Text Delivery/Postal/On-line | |||||
| Cared for appropriately with dignity, compassion and respect (Strongly Agree/Agree) | |||||
| Q1 | Q2 | Q3 | Q4 | YTD | |
| PTS | 90.50% | 94.20% | 95.40% | 94.70% | 93.40% |
| PES | 92.60% | 89.70% | 89.60% | 90.30% | 90.60% |
| UCS | 92.60% | 91.60% | 95.20% | 94.80% | 94.00% |
| 111 | 94.50% | 97.10% | 92.50% | 95.70% | 94.10% |
Table: Percentage of respondents who strongly agree/agree they were cared for appropriately with dignity, compassion and respect.
| Patient Engagement Surveys SMS Text Delivery/Postal/On-line | |||||
| Overall Satisfaction Received (Very Satisfied/Fairly Satisfied – Yes) | |||||
| Q1 | Q2 | Q3 | Q4 | YTD | |
| PTS | n/a | n/a | n/a | n/a | n/a |
| PES | n/a | n/a | n/a | n/a | n/a |
| UCS | n/a | n/a | n/a | n/a | n/a |
| 111 | 87.40% | 87.00% | 85.10% | 89.90% | 86.90% |
Table: Percentage of respondents who were very satisfied/satisfied overall with their care
| Patient Engagement Surveys SMS Text Delivery/Postal/On-line | |||||
| Overall Experience of Service / Recommend Ambulance Service to Friends and Family (Very Good/Good – Extremely likely/Likely) | |||||
| Q1 | Q2 | Q3 | Q4 | YTD | |
| PTS | 89.10% | 91.00% | 92.10% | 91.50% | 90.70% |
| PES | 91.30% | 90.10% | 88.20% | 91.10% | 90.20% |
| UCS | 84.30% | 74.80% | 81.40% | 81.80% | 82.20% |
| 111 | 89.70% | 90.00% | 88.00% | 89.20% | 89.10% |
Table: Percentage of respondents who would recommend the ambulance service to family and friends
It should be noted the fields above showing ‘not applicable’ indicate that the question was not included in that survey.
Examples of additional narrative in feedback include:
“Excellent, amazing service. Extremely professional. My son is autistic, and the two paramedics went the extra mile to make sure reasonable adjustments were made to aid his recovery, kind understanding and valued my input so to get full picture of events and past history. Couldn’t have asked for more in an already stretched area of the NHS. Excellent.” (PES).
“Excellent staff very caring and kind. Just what you need after outpatients’ treatment. I truly appreciate this vital service. Thank you all. PS. Also the lady on the phone taking the booking was kind and caring and made it so easy for me. That too was greatly appreciated.” (PTS)
“Both paramedics were empathetic, conscientious, thorough and my partners symptoms were taken seriously in spite of them being less serious than he initially thought. We did not wait an excessive amount of time. Overall, a very reassuring/supportive experience. Credit to both paramedics and the practitioner who took the 111 calls.” (PES).
90.2% of PES patients, 86.9% of NHS 111 patients and 90.7% of PTS patients also found their overall experience of the respective services either good or very good.
“My Mum travels to and from dialysis by ambulance three times a week. She is 86 and quite frail and can get a bit confused. All of the ambulance crews have taken the time to get to know her well and they are all so kind, caring and professional in their dealings with her. They have a chat and a joke with her and she loves them all.” (PTS)
“Amazing service from NWAS. Ellie and the team were super with my Mum who had fallen and were really kind and compassionate. They were very thorough and quickly examined my Mum, giving excellent treatment and a real human touch. They were calm, quick acting and efficient. Really went the extra mile. Thank you all so much again, really grateful for your amazing service at a very stressful time. It is really appreciated.” (PES)
“111 knew my husband needed help. They took control of his problem. They got an ambulance to take my husband to the urgent care centre, he was treated straight away, on monitors, admitted to hospital. I can’t thank 111 enough, as I was panicking. They knew the situation and responded. Ambulance service, 111, all amazing. If it wasn’t for 111, my husband would not be alive today. They took complete control and responded by saving my husband’s life. We are eternally grateful.” (NHS 111)
Friends and Family Test (FFT)
PTS and PES ‘see and treat’ patients receive the opportunity to provide FFT feedback monthly through an SMS message. Monthly FFT data is shared via IPR at Board, Quality and Performance Committee and nationally with NHS England. A thematic analysis of the FFT qualitative feedback continues to show a high regard for the professionalism, care and compassion shown by our staff. Areas of learning include delays, waiting times, and where there could be expectations for some of our more vulnerable PTS patients when using third party or bariatric services and wheelchair support.
The table below provides a breakdown of the FFT feedback data and channels used to gather patient experience. As can be seen, a high number of patients provide qualifying narrative to support their response.
| 2024 – 2025 Summary of FFT Responses and Channels | |
| FFT responses received in 2024 – 2025 | 22,394 |
| Increase compared to 2023 – 2024 | 26.14% |
| Additional comments entered on FFT responses | 17,982 |
| SMS text survey responses | 89.14% |
| Postal postcard surveys | 2.85% |
| On-line responses | 8.01% |
Table: Breakdown of FFT responses and channels
Demographic analysis of patient survey and SMS FFT respondents
The table below shows the percentage breakdown of survey respondents by demographics for our PTS, PES, urgent care service and NHS 111 surveys, and where we received FFT feedback via SMS on our PES and PTS service lines. Some key headlines show:
- 95.3% of PTS respondents are over 45 years of age.
- 58.9% of NHS 111 respondents are female.
- 82.8% of PTS respondents declared a disability.
- An average of 6.22% of all respondents were from ethnic minority communities.
- On average, 1.73% of all respondents preferred not to declare their ethnicity.
A continued focus for 25/26 will be to increase the amount of feedback we receive from mixed ethnic communities and to improve the capturing and reporting of demographic information and protected characteristics.
| Patient Transport Service (PTS) | Paramedic Emergency service (PES) | Urgent Care Service (UCS) | Localised 111 | National 111 | PTS Friends & Family Test (FFT) | PES Friends & Family Test (FFT) | ||
| Mode of correspondence | (URL) | (URL) | (URL) | (URL) | (Postal) | (SMS Text) | (SMS Text) | |
| Patient Age | Under 16 yrs | 0.6% | 6.8% | 5.2% | 18.2% | 3.7% | 0.9% | 1.2% |
| Over 16+ yrs | 99.4% | 93.2% | 94.8% | 81.9% | 93.8% | 99.1% | 96.4% | |
| Over 25+ yrs | 99.1% | 90.7% | 90.0% | 76.0% | 91.2% | 98.5% | 93.6% | |
| Over 35+ yrs | 98.5% | 86.2% | 83.8% | 63.0% | 85.3% | 97.4% | 89.0% | |
| Over 45+ yrs | 95.3% | 79.7% | 76.3% | 51.0% | 76.8% | 94.4% | 78.8% | |
| Over 55+ yrs | 86.6% | 69.5% | 66.1% | 34.8% | 69.1% | 86.5% | 65.1% | |
| Over 65+ yrs | 65.6% | 53.2% | 50.1% | 16.2% | 55.2% | 67.7% | 42.6% | |
| Over 75+ yrs | 36.3% | 32.8% | 32.2% | 5.1% | 32.6% | 41.3% | 21.9% | |
| Over 85+ yrs | 8.5% | 9.2% | 10.8% | 0.8% | No data | 12.2% | 6.7% | |
| Patient Gender | Female | 53.2% | 53.1% | 58.9% | 57.7% | 60.3% | 55.0% | 60.3% |
| Male | 46.6% | 46.4% | 40.7% | 41.9% | 37.5% | 45.0% | 36.7% | |
| Prefer not to say | 0.2% | 0.6% | 0.4% | 0.4% | 2.2% | 0.0% | 3.0% | |
| Patient Impairment | Limiting illness | n/a | n/a | n/a | n/a | 47.6% | n/a | n/a |
| None | 17.2% | 41.2% | 46.3% | 68.2% | 47.0% | 6.3% | 37.9% | |
| More than one | n/a | n/a | n/a | n/a | n/a | 26.9% | 18.2% | |
| Mobility | 68.3% | 37.2% | 31.3% | 15.5% | n/a | 52.3% | 20.4% | |
| Hearing | 14.9% | 14.9% | 13.6% | 4.6% | n/a | 0.8% | 2.1% | |
| Visual | 8.9% | 5.9% | 4.5% | 0.4% | n/a | 3.2% | 0.7% | |
| Mental Health | 10.7% | 15.2% | 17.2% | 10.5% | n/a | 2.0% | 7.7% | |
| Dementia | n/a | n/a | n/a | 0.0% | n/a | 0.8% | 2.7% | |
| Learning | 1.7% | 3.0% | 4.7% | 3.8% | n/a | 0.8% | 1.3% | |
| Don’t know | n/a | n/a | n/a | n/a | 2.0% | 0.8% | 1.3% | |
| Prefer not to say | n/a | n/a | n/a | n/a | n/a | 6.9% | 9.2% | |
| Patient Ethnicity | (Black & Minority Ethnic Communities) | 3.9% | 5.0% | 7.3% | 8.3% | 6.1% | 5.4% | 7.6% |
| Prefer not to say | 1.7% | 1.2% | 0.8% | 0.8% | 0.0% | 2.7% | 3.2% | |
Table: Percentage data breakdown of 24/25 respondents by demographics
Reporting
Friends and Family Test patient feedback is reported monthly to the board through the Integrated Performance Report and quarterly via the Communications and Engagement team dashboard. Key engagement themes and initiatives are also shared with the Quality and Performance Committee, while Equality Diversity and Inclusion (EDI) updates go to the EDI Sub Committee.
In 24/25, we continued quarterly service improvement dashboards and began developing a new, combined patient feedback dashboard—an important initiative that will continue into 25/26.
Feedback themes.
Feedback over the year has consistently demonstrated a generally high regard for the ambulance service and in particular, the high percentage of patients feeling they were treated with dignity, compassion and respect (92.8% of survey respondents).
Some of the themes and feedback highlighted during the year have included:
- Awareness of the NHS 111, online services for those from ethnic minority groups
- Awareness of the availability of interpretation and translations services for deaf, black and ethnic minority communities (BAME).
- An understanding of what information may be requested when 999 is called for patients whose first language is not English.
- Profiling job roles, routes to employment and volunteering within the ambulance service at our community events.
- Increased understanding of how to improve services for patients with a learning disability or autism, including the opportunity to learn basic British Sign Language (BSL).
- Staff awareness of cultural and religious differences when entering homes and the ability to provide dignity in death.
Patient and Public Panel – Giving our patients ‘an increased voice’
Our volunteer Patient and Public Panel (PPP), established in 2019, is made up of representatives from local communities, interest groups, the voluntary sector and partner organisations. It provides meaningful opportunities for members to influence decisions and identify improvements in our urgent and emergency care, patient transport, NHS 111 and back-office services, in a way that suits their lifestyle and the time and commitment they are able to give. Panel members bring expert lived experience and knowledge of our services, and offer valuable insights into numerous projects, initiatives, policies, systems and campaigns.
The PPP has a flexible infrastructure to enable patients/the public to become involved at one or more levels that best suit them. All levels are equally important and consist of:
- ‘Consult’ is virtual, making the most of digital channels to interact with members
- ‘Co-produce’ panel members work together on short-term projects
- ‘Influence’ members take an ongoing, active role in high-level meetings.
A breakdown of PPP member’s involvement by level can be found below.
Figure: Breakdown of PPP involvement by membership level
As our PPP has continued to grow over the last 12 months, we have actively engaged with our members via both face –to face and virtual platforms with the intention of ensuring our members feel supported in the role. Our 344 PPP members are fully inducted into the organisation, with many already involved in work with the trust.
The table below shows the distribution of PPP members across the localities.
Figure: Breakdown of member locality
During 24/25 we increased the diversity of the panel’s membership, rising from 24% to 26% for cultural representation, 32% for youth representation and 25% for representation of patients with disabilities. The panel’s feedback and lived experience are invaluable to the trust to better understand our patients’ experience, produce stories, analysis and themed findings which in turn inform service development.
Figure: Age PPP members
In 24/25, PPP members have been invited to join a variety of forums with 23 requests for panel involvement from staff across the trust, as well as external partners such as Lancashire and South Cumbria Integrated Care Board. Areas the PPP have been involved in include regular attendance at high-level meetings such as area learning forums, attendance at trust board and Learning from Deaths. In addition, our PPP have played a significant role in forming strategy, developing resources and supporting projects, including the removal of existing medical markers, Quality Improvement Academy, Trust Strategy review and linguistics during 999 calls.
Panel members receive regular information via a weekly roundup newsletter, with 51 editions shared during 24/25. Some of the featured articles included Black History Month, World Menopause Day, PPP session looking at 999 calls and linguistics, and an invite to attend a Cardiac Prevention Awareness Event organised by the Jewish Community Foundation. There are also opportunities for members to engage with each other on a dedicated PPP members’ area of the trust’s website.
During 25/26, PPP members will be invited and recognised for their contribution in a dedicated event for all our trust volunteers due to be held in October/November 2025.
A summary infographic containing our achievements across 24/25 will be produced and shared with PPP members.
Patient, Public and Community Engagement
Whilst patient surveys provide us with a real insight into the care and treatment that patients have received, another method we use to gain qualitative feedback is by engagement with community and patient groups within our region. Our focus has been to reaffirm the basics of what we offer across each of our three main service lines and to explore any misconceptions and/or barriers to access. We have also used these valuable face –to face opportunities to educate our communities about self-care, winter health messaging and offer service based activities to elicit their understanding and experience of care.
During 24/25 we attended nine virtual engagement events, and 22 face –to face engagement sessions which were attended by the trust as principal speakers, advisors or facilitators. These events included the Kashmir Youth Project, Wirral Multicultural Organisation, Greater Manchester Faith forum, Wai Yin society and the Chinese Wellbeing group in Liverpool.
Further support is provided to our patient groups upon request, for example supporting cardiopulmonary resuscitation (CPR) training. Examples of the groups we have supported include the Liverpool Chinese Students and Scholars Association (LCSSA) and the Chinese Wellbeing group in Liverpool. This work will continue with the British Islamic Medical Association (BIMA) and the Lancashire Council of Mosques during 25/26.
In addition to this we have also been able to support 29 high attendance events in 24/25. Examples include PRIDE, university freshers events, Greater Manchester Ethnic Communities Network Event, a cardiac prevention Event within the Jewish community and the Liverpool Chinese Students and Scholars Association (LCSSA) Spring Festival Gala. Our engagement with the Jewish and Chinese community has considerably increased this year due to our continued focus and support.
Targeted work with young people, including oversees students, provides an opportunity to offer information about accessing NHS services. In addition, it has provided individuals with an opportunity to explore volunteering and career opportunities within the ambulance service or the wider NHS.
We will continue our face-to-face attendance during 25/26 at health melas, PRIDE etc and are looking to expand our attendance and engagement with a range of under-represented black and minority ethnic communities.
Protected characteristics
The Equality Act 2010 identifies nine protected characteristics cited as: age, disability, gender reassignment, race, religion or belief, sex, sexual orientation, marriage and civil partnership, and pregnancy and maternity. During 24/25, we have engaged with people who have identified as having a protected characteristic. The graph below shows the number of people we have engaged with who identify as having a protected characteristic.
Protected characteristics of patient groups engaged during 24/25
Figures: Groups protected characteristics 24/25
Quality Improvement initiatives with underrepresented groups.
Our Patient Inclusion team has established a task and finish group to ensure under-represented voices are included in decision-making.
As part of this work, we’ve begun engaging with Chinese and Jewish communities in the North West through focus groups. These sessions aim to understand their experiences, expectations, and any barriers to accessing our services. Feedback will help identify gaps in representation and drive meaningful improvements.
Ambulance Awareness Day events
Over the past year, we successfully delivered five county based face –to face community awareness events. Our Greater Manchester event, held alongside the trust’s Annual General Meeting, featured information stands from NHS 111, PES, PTS, and corporate staff, as well as CPR training sessions. It attracted 203 attendees—66% from ethnic minority backgrounds, 15% from the Chinese community, and 40% aged 16–24.
In Cumbria, Lancashire, Cheshire, and Merseyside, Ambulance Awareness Days used interactive tabletop exercises and themed speakers to raise awareness, gather feedback, and discuss PES, PTS, and NHS 111 services. These activities helped identify what’s working well and where improvements are needed. Based on feedback, we developed a snapshot of service improvements and an accessible summary document, shared with attendees in August 2024 and published on our website. Some activities also supported winter demand planning—for example, NHS 111 tables addressed common concerns like repeat prescriptions during public holidays, supported by useful giveaways and leaflets.
We select event venues in areas frequently used by local communities, often where health outcomes are poorer. This has helped us reach groups that are typically harder to engage. Attendee demographics are shown below. Feedback summaries and planned improvements are shared with attendees and community groups, and this approach will continue into 25/26 as we review future event locations.
Figure : Groups identifying with protected characteristics attending the ambulance awareness day events.
Examples of feedback themes received from events include:
- Staff very friendly, enjoyed the CPR training, and HART stand
- Very good event, very satisfied with the stalls and activities on offer
- Good development for any PPP member, great opportunity for the community, excellent practical exercises
- NWAS dyslexia support for existing staff and recruitment.
- Good information on how to deal with mental health calls.
- Helpful information on how to support patients whose first language is not English, including basic British Sign Language (BSL) training available to operational staff.
- Information on how to find a patient from a mobile number calling 999.
Filmed patient and staff stories
Filmed patient and staff stories remain a powerful tool to highlight real experiences and share learning. These are presented bi-monthly to the NWAS Board of Directors and Quality and Performance Committee, including staff training, and featured in education and awareness campaigns. In 24/25, patient stories covered topics such as STEMI (Segment Elevation Myocardial Infarction) response times, heart condition pain awareness and winter pressures. Staff stories during the year include the ‘HALO Project’ (redefining the ambulance liaison officer role); the Care Home Engagement Project and Aspirer welfare initiative.
Patients’ experience recommendations and improvements
Feedback themes gathered from all the approaches the trust uses to listen to, engage and seek patient experiences are used to inform recommendations for improvements. The team produces learning dashboards for PTS service improvement ambassadors to share feedback and learning, and ensure support for the co-design of service improvements within the trust. This approach will be enhanced with learning dashboard availability on PES and NHS 111 services during 25/26.
Some of our recommendations and improvements include:
- Feedback shared by the Chinese community highlighted the lack of awareness with the services we provide and fear of not being able to communicate in their spoken language. We have translated our 999 and PTS leaflets into Cantonese and Mandarin and are producing a film to demonstrate how we can communicate with patients in their spoken language – this will inform a patient story to be shared within the trust.
- Feedback shared by Lancashire School of Mosques highlighted the importance of ambulance staff wearing shoe coverings when entering a Muslim patient’s home. We produced a written piece for our staff weekly bulletin and included this information on our staff intranet page which all of our staff have access to. This ‘you said we did’ was further communicated with Lancashire School of Mosques and our monthly newsletter.
- Feedback was also shared at one of our community events in relation to staff considerations when entering homes. Further to this, during the year, we launched our NWAS Religion, Belief and Culture Card. Key areas covered in the card are: some of the most likely first languages that are used by patients from different religious beliefs residing in the North West to improve staff communication, cultural norms with physical contact and customs with dying and death informing our approach to end –of life care.
- When engaging with patient community groups on NWAS services, feedback has shown an increase in requests for CPR training and a need for further understanding and awareness raising on DNACPR (do not attempt CPR resuscitation). We will ensure these CPR requests are actioned appropriately and build capacity to increase understanding of DNACPR information into our community engagement plans.
- Our Ambulance Awareness Day events format changed during 24/25 based on feedback from our attendees. A knife incident related scenario and mental health related talks are now included in the event programme. We will continue to regularly share information on mental health support available in each county area via our community info burst newsletters.
- Initial approaches were made to the trust’s research and development and the widening access team to support with 3D virtual reality ambulance viewing headsets for use at our ambulance awareness day events. These proved to be very popular mainly with young people that attended the events. We will continue to work together with the widening access team to ensure these are available for future events.
- A discussion was held with PPP members as to what they think should be included in the trust Mental Health and Dementia Strategic Plan for 2024-2027. The trust Mental Health leads team will be producing a separate plan for dementia and will be coming back to the PPP to help produce this plan along with other plans in the future.
- PPP members reviewed our pictorial e-book to help ensure each question and procedure within the book is clearly explained to support neurodiverse and learning disability patients. Feedback shared from PPP members resulted in some of the terminology changing to make it easier to read and additional questions included to help neurodiverse and learning disability patients when being treated.
- Our PPP charter has been reviewed and now includes key information for our PPP members when attending trust meetings and what they can expect from us to keep them informed and supported fully as members. The reviewed PPP charter will be launched and sent to the membership early 25/26 through the PPP newsletter.
- Our PPP forum is not frequently accessed by PPP members. We will consult PPP members on how the forum can be better utilised including any changes to the layout to make it more accessible and easier to use.
- Further to a variety of requests from ICB commissioners for PPP support with some of their projects and initiatives, further development training will be sourced for PPP members to enable them to confidently get involved with high level projects and meetings.
- A summary infographic containing our achievements across 24/25 will be produced and shared with PPP members.
- Patient Engagement colleagues to undertake facilitator training to support with leading on conversations and group discussions at external events.
- We will promote our attendance at community engagement events using scheduled social media channels to highlight where patients and groups can meet us.
- Targeted attendance with schools and colleges has ensured all our Ambulance Awareness Day events are well attended by a young generation considering pursuing a career in the ambulance service. We will continue to build on this with profiling job roles, routes to employment and volunteering within the ambulance service at our community events during 25/26.
- Our PTS Level 2 learning dashboard data enables the sharing of patient feedback, promoting best practice and boosting staff morale. During 25/26, we will ensure that PTS managers highlight this data on all NWAS stations that have visual display screens.
- Increased survey feedback from underrepresented groups will ensure the development of demographic feedback into our digital platforms – this will be supported by additional outreach to increase survey feedback from black, Asian, and minority ethnic (BAME) communities.
- Feedback from our deaf communities continues to share concerns and barriers to accessing our services. As a result, we will produce an ‘Insight App’ film for operational staff awareness with using language and BSL interpreters at patient side. We will also feature the Blue Light Academy basic sign language training as part of this work.
- To support frontline staff awareness with the various accessibility tools available, we shared a staff bulletin signposting this information on our trust intranet the ‘Green Room’. We will continue to review and update this information annually.
- Easy read formats of our service information are provided to Ambulance Awareness Day event attendees with learning difficulties. Further work will include an easy read production of the event evaluation form. Alternative format is ensured in our regular communications with our communities in all publications including monthly info-bursts and PPP weekly round ups.
- A health literacy improvement project will also see the creation of new, accessible information for patient transport service users.
- A regular programme of filmed staff and patient stories is produced and shared with the board and used for learning within the trust.
Management of Complaints 24/25
Complaints are managed by the Patient Advice and Liaison Service (PALS) and Resolution team, who ensure open and honest investigations are aligned with relevant legislation and the Model Complaint Handling Procedure, as outlined by the Parliamentary and Health Service Ombudsman (PHSO). Our goal is to achieve satisfactory resolution for complainants, while maintaining compliance with best practices.
NWAS remains steadfast in its commitment to delivering a high-quality and patient-centred complaint experience. We recognise the importance of concerns, complaints and feedback as essential tools for continuous improvement. Insights from patients, their families, and service users allows us to assess our practices, identify areas for enhancement, and implement necessary changes at both individual and system wide levels.
The PALS and Resolution team ensures that individuals who raise concerns feel heard and that their complaints are addressed effectively. 24/25 saw specific focus on evolving our responses to complaints, making sure that letters and communications are patient centred, and always demonstrate empathy and compassion. The PALS and Resolution team continue to address complaints with fairness and transparency, with the end goal being to improve a patient’s experience and drive service improvement.
Governance and Reporting
The board of directors receive information on complaints through a structured reporting framework:
- Bi-monthly reporting: Complaints data and insights are included in the integrated performance report presented to the board.
- Quarterly Assurance Reports: The Quality and Performance Committee review these reports to ensure accountability and oversight in line with complaint standards and legislation, volume of complaints received, team performance and tracking any themes of learning.
- Reportable Events Paper: Complaints raised to the Parliamentary Health Service Ombudsman are reported in this paper and include information about decision rationale, outcome and actions recommended by the independent reviews.
- Clinical Quality Group: This group is chaired by the Medical directorate and clinical complaints are reported to provide assurance relating to the safety and quality of all clinical activities within the trust across all services lines.
- Area Learning Forums: These forums discuss actions resulting from complaints and oversee implementation through structured action plans.
Through these assurance groups and committees, we ensure that patient feedback is not only acknowledged, but also used constructively to highlight the patient journey and identify recurring themes or trends in complaints. These insights are addressed with appropriate actions, providing assurance that improvements are made where needed.
Complaint Figures
2,277 complaints were raised with NWAS last year and 89% of these were recorded as ‘low complexity’ complaints, managed by the Patient Advice and Liaison (PALS) team. The PALS team guide appropriate and empathetic apologies within an everyday conversation, as guided by the PHSO’s standards.
The three most common themes of complaints received, across the range of low, medium and high levels of complaints, related to:
- Care and treatment
- Delays
- Call handling
Care and treatment
The table below shows the number of complaints about care and treatment managed at each level of complexity.
| High complexity | Medium complexity | Low complexity | Total |
| 20 | 113 | 781 | 914 |
Table: Number of complaints about care and treatment complexity levels.
A full breakdown of the sub-categories shows the specific category of treatment complaints, raised with NWAS.
| Sub-type of complaint | Number of complaints |
| Professional standards (conduct) | 619 |
| Disposition | 165 |
| General | 79 |
| Clinical treatment | 42 |
| Equality | 6 |
| Assessment | 3 |
Table: Category of complaints.
The complaints regarding care and treatment by service line and area, may vary from the total number provided above, as a singular complaint, may involve multiple service lines.
| Service line | Number of complaints |
| Patient transport service | 268 |
| Greater Manchester, paramedic emergency service (PES) | 199 |
| Cheshire and Merseyside (PES) | 181 |
| Cumbria and Lancashire (PES) | 164 |
| NHS 111 | 113 |
| Emergency operations centre | 48 |
Table: Care and treatment complaints by service line.
Delays
734 complaints were raised with us about a delay in service. Below, outlines the complexity level assigned to each complaint.
| High complexity | Medium complexity | Low complexity | Total |
| 9 | 33 | 692 | 734 |
| NWAS service line | Number of complaints |
| Paramedic emergency service (PES) | 585 |
| Patient transport service (PTS) | 149 |
Table: Complexity level by service line – delays.
Call Handling
364 complaints were raised about an aspect of the call handling part of a patient’s journey with NWAS.
| High complexity | Medium complexity | Low complexity | Total |
| 7 | 33 | 324 | 364 |
[
| NWAS service line | Number of complaints |
| NHS 111 | 166 |
| Paramedic emergency service (PES) | 155 |
| Patient transport service (PTS) | 43 |
Table: Complexity level by service line – call handling.
Complaint Outcomes
2,242 complaints were closed in 24/25 with 86% of all complaints closed within local Service Line Agreement, an improvement on the 81% closure within local Service Line Agreement achieved in 23/24.
| Complaint outcome | Complaint level | Total | |
| Upheld | High | 15 | 622 |
| Medium | 53 | ||
| Low | 554 | ||
| Not upheld | High | 11 | 928 |
| Medium | 88 | ||
| Low | 829 | ||
| Partly upheld | High | 5 | 692 |
| Medium | 57 | ||
| Low | 630 | ||
Table: Complaint outcomes 24/25
Parliamentary and Health Service Ombudsman
In 24/25, NWAS received 10 notifications from the Parliamentary and Health Service Ombudsman (PHSO) regarding complaints submitted for independent review.
- Three cases were closed following an initial assessment, with no failings found on the part of NWAS.
- Two cases were resolved through mediation or further local review and subsequently closed.
- One case was not upheld, with the PHSO identifying no failings by NWAS.
- One case was partly upheld, resulting in a recommendation for further apologies to be offered to the complainant.
Three cases remain open as we move into 25/26 and are currently under detailed investigation by the PHSO.
Freedom to Speak Up
We are committed to an open and honest culture, maintaining high standards of patient care, continuously striving to act honestly and with integrity in our approach to management systems, processes, responsibility as an employer, protecting the people who work within the organisation and communities that it serves from harm.
Freedom to Speak Up Activity 24/25
In addition to speaking up through leadership teams and normal workforce processes, we have established well embedded additional speaking up processes to create a culture of safety. We continue to foster a workplace where our people feel safe to speak up and raise concerns. This in turn allows us to provide highly effective care where we learn when things might not go well. Our team of Freedom to Speak Up (FTSU) guardians have this year seen a reduction of 21.4% in the number of concerns raised (121 from 154 in 23/24).
Ambulance services, in line with other blue light services, have come under increased scrutiny from the national media along with NHS England. The Thirlwall Inquiry prompted a comprehensive review of all NHS speaking up arrangements.
This year has seen 121 concerns raised with the FTSU guardians, categorised into themes according to the National Guardian’s Office (NGO) returns.
| Themes | Percentage | Number |
| Inappropriate attitude and behaviours | 61.2% | 74 |
| Patient safety | 15.7% | 19 |
| Bullying and harassment | 13.2% | 16 |
| Worker safety | 6.6% | 8 |
| Fraud | 0.8% | 1 |
| Detriment | 2.5% | 3 |
Table: FTSU themes 24/25
The proportion of patient safety concerns has decreased. We have focused on the many ways in which staff can raise any concerns from informal/formal discussions with local mangers and leaders through to formal paths such as Grievance/Dignity at Work process and safety concerns raised through our Incident reporting system.
Through a formal leadership development program, leaders are equipped to make themselves ‘open’ to discussion and actively listen to staff concerns. This enables leaders to negotiate positive outcomes that meet the staff needs and addresses their concerns whilst also considering impacts on all staff, patients and the organisation.
We have instigated several new processes to ensure we deal with concerns in a consistent way, ensuring an impartial view which supports both staff and managers to resolve concerns using learning. This reflects in the feedback we have received from staff and managers who have been involved with FTSU guardians.
Our Quality Account 24/25 provides further detail in relation to Freedom to Speak Up.
Exercise of functions in relation to health inequalities
Background
NHS England’s statement on information on health inequalities (duty under section 13SA of the National Health Service Act 2006) was published on the 27 November 2023, describing the powers available to relevant ICBs, NHS trusts and NHS foundation trusts to collect, analyse and publish information in relation to health inequalities, and NHS England (NHSE) views about how those powers should be exercised in connection with such information.
The duty to report information on health inequalities will encourage better quality data, completeness and increased transparency. The expectation from NHSE on how the statement will help address health inequalities is that by having good quality, robust data, this will enable NHS organisations:
- To understand more about the populations they serve
- To enable identification of groups that are at risk of poor access to healthcare, poor experiences of healthcare services, or outcomes from it
- Deliver targeted action to reduce healthcare inequalities.
As per the statement, NWAS is required to review the extent to which the trust has exercised its functions consistently to the statement, and to include a report as part of our Annual Reports 23/24 and 24/25, aligned to the trust’s annual reporting guidance. The statement requires relevant organisations to:
- Publish a list of pre-defined indicators disaggregated by age, sex, deprivation and ethnicity, aligned to the five priority areas for addressing healthcare inequalities set out in the 23/24 priorities and operational planning guidance and the Core20PLUS5 approach for adults and children and young people.
- Report other information on health inequalities relevant to local populations or priorities as they consider appropriate and at their discretion.
In relation to point one and as reported in last year’s Annual Report, NWAS does not collect nor report on any of these indicators as these relate to acute trusts and GP data. For completeness and illustration, the list of indicators in Appendix 1 of NHSE statement can be found here: https://www.england.nhs.uk/wp-content/uploads/2023/11/PR2128-i-nhs-englands-statement-on-information-on-health-inequalities.pdf
The main content in this section provides information on data activities carried across the trust in relation to point two, including collection, reporting, publication or sharing, and analysis to derive insights to help deliver targeted action.
Data collection
NWAS continues to engage with partners and to assess internally how to improve collection of patient demographic characteristics, focusing initially on those requested as per the statement’s first publication: age, sex, deprivation and ethnicity. Current NHS Spine interoperability allows transfer of age and sex patient’s data, but not ethnicity, which is a challenge across NHS organisations. NWAS staff took part in the ‘Improving Ethnicity Recording Workshop’ organised by NHSE North West region and the Association of Directors of Public Health London on 16 January 2025. This workshop resulted in the creation of the NHS Futures ‘Improving Ethnicity Recording Collaboration workspace’ to connect, collaborate and contribute to the co-creation of dynamic approaches to impact recording of ethnicity and share examples of successful approaches. Similarly, NWAS supports AACE’s ongoing conversations with NHS England to enable sharing of centrally recorded patient ethnicity data with ambulance services for both, direct care and secondary use purposes.
Following internal analysis by the Public Health team, the ethnicity data across service lines at NWAS is as follows:
- Analysis of 980,084 incidents attended by 999 PES between April 2023 and March 2024 showed 61.6% of records have an ethnicity category other than null or unknown, of these, 58.6% have white ethnicity.
- Preliminary analysis of 1,255,861 PTS April 2022 – March 2023, showed 5% of patient transport service journeys have an ethnicity category in records.
- Based on 1,942,281 calls from 111 between March 2024 and March 2025, 94% of 111 calls collected ethnicity data.
The high completion percentage of ethnicity data in 111 calls is due to well-embedded training processes, which is enabled by the nature of the service. For 999 data, the Digital Innovation and Integration team has explored retrospective completion of ethnicity data linking 111 patient data to 999, but this approach has been paused on anticipation of the national solution pursued by AACE. For PTS, given the ongoing tendering process and other improvement work already taking place, there are no immediate plans to initiate a project to improve ethnicity collection, but this will be revisited in the new year.
Collection of patient characteristics in feedback received by patients and members of the public continues to be an area of priority for the Patient Engagement team. This year, DCIQ and complaints reports started mandating collection of patient characteristics data. Additionally, the Clinical Audit team is commissioning of a new Clinical Audit Tool, with requirements including facilities to capture and report on patient demographic data.
Separately, in relation to data collected on incidents where violence took place, the Violence Prevention Reduction and Security team have improved collection of aggravating factors, enabling staff to capture subjective data on whether ethnicity, age, gender, gender preference, mental health conditions or other factors such as intoxication or medical condition, played a role in violence incidents. Violence towards staff during the conduct of their duties is an issue of high importance for ambulance services as evidenced by the 2024 NHS Staff Survey results, which indicates that amongst health care workers, the percentage of ambulance staff who report experiencing one or more incidents of physical violence from patients, relatives or members of the public is more than double the national average for all healthcare workers, 30.6% in comparison to 14.4%, respectively.
The last of the four data characteristics requested in the statement is deprivation. Before this year, index of multiple deprivation was captured on an ad-hoc basis for some reports. This year the Business Intelligence team implemented a technical solution to link population level data to the postcode of recorded incidents, enabling population of the index of multiple deprivation (IMD), decile or quintile for each record. This linkage has started for 999 service line records, but it is envisaged that this will be rolled out to other service lines in future.
Data reporting
This year, as per the Sustainability Strategy’s population health objective to improve the input, analysis and utilisation of data to provide intelligence on population health and health inequalities, and driven by the requirements from NHS England statement on health inequalities, the Public Health team developed a specification for a set of dashboards to provide a demographic breakdown of our service lines data by patient characteristics and population health characteristics. This initial specification comprised the following priorities:
- To identify the drivers of NWAS activity in the population based on 999, 111 and patient transport services.
- To identify the drivers of demand for the “CORE20” group across our services and across our region.
- To identify the priority groups within the North West population (this refers to the ‘plus’ groups as per the CORE20PLUS5 framework; which includes ethnic minority communities; people with a learning disability and autistic people; people with multiple long-term health conditions; or other groups experiencing social exclusion, known as inclusion health groups.
- To develop indicators to measure the NHSE health inequalities indicators as appropriate for ambulance services.
NWAS made a substantive commitment to allocate Business Intelligence resources to development of phase one of this work. This phase aimed to address specification priorities one and two for 999 service data. As a result, the Public Health team and the Business Intelligence team delivered NWAS’ first Power BI population health dashboard to report on 999 calls and face –to face incidents records. An example of a view from the dashboard is shown below:
Screen shot of the Power BI dashboard showing NWAS statistics relating to Burnley
Our Annual Plan for 2025-26, includes a deliverable to work on phase two. Alongside development of phase two, we will work towards developing our understanding of the insights provided by the initial dashboard, using these insights to identify opportunities for actionable projects to support the reduction of health inequalities, working in collaboration with system partners. Importantly, the work completed to develop the dashboard will enable new analyses of 999, 111 or patient transport services data to identify differences across protected characteristic groups of areas of deprivation. Together, this work will help us identify if inequalities exist, report findings to the Board and partners, and enable conversations to tackle these differences in care.
In relation to internal reports, the board continues to receive Learning from Deaths reports which include demographic breakdown of incidents by age, sex, ethnicity and deprivation. This year, the Complaints team embedded monitoring of patient characteristics into reports to learn from complaints and patient safety incidents, so protected characteristics are now captured within complaint logs (DCIQ) and the Complaints team is able to extract for reporting purposes.
Data publication or data sharing
Externally, we continue publication of Learning from Deaths quarterly reports, as well as the annual Patient Engagement Report, both reports include age, gender, and ethnicity. The Learning from Deaths report includes deprivation information, whereas the Patient Engagement Report includes information on patient disabilities. NWAS has sharing agreements to transfer activity and patient data with our local, regional and national system partners, including, for instance, data on violent incidents with the Trauma and Injury Intelligence Group (TIIG) to help inform prevention efforts. The Information Analytics team has a process in place to share data with external parties to request NWAS data, this could be for public or private purposes, and subject to data protection requirements. For public purposes, specifically in relation to help inform prevention programmes. This year the team served requests in relation to public health priorities, including data on intoxication through vaping, suicide attempt incidents, and falls.
Nationally, NHSE developed the national Ambulance Data Set (ADS) to increase understanding of why people use ambulance services and how ambulance services deliver urgent and emergency care. The dataset will provide consistent level of detail about how ambulance services nationally respond to and treat 999 calls. This data set will enable linkage with the Emergency Care Data Set (ECDS) providing a more complete picture of how and why people access urgent and emergency care, as well as of patient outcomes, safety and experience, and includes data of patient characteristics. NWAS is submitting data from our calls (CAD) and our face –to face incidents responses (EPR) as per national requirements.
On a project basis, as described in more detail in the Public Health team section in the report, NWAS is working with system partners to develop their understanding of how NWAS can support integration at a local and regional level, for instance, through integration with local authorities commissioned drug cessation and support services to support patients with non-fatal drug overdoses, and through integration with primary care partners to leverage routinely collected ambulance data to support secondary prevention of long-term conditions.
Data analysis and use of insights to deliver targeted action
Following the recent completion of phase one of the population health dashboard, a brief overview of the initial insights derived from this work are provided. As part of the work to develop the specifications for the population health dashboard, the Public Health team conducted a preliminary analysis of 999 EPR records, face –to face incidents attended in the period April 2023 – March 2024. This analysis, together with initial insights from the dashboard provide the top reasons for NWAS calls and ambulance attendances at a region level, which are chest pain, dyspnoea, abdominal pain and seizure. To note that there is a small difference between falls and chest pain rates. When analysing demand from incident locations in the quintile of highest deprivation, the top reasons for calls are the same but chest pain comes top with a considerable difference between this and the next reason, falls. Of interest, the sixth top reason for calls and incidents attended for the quintile of lowest deprivation, is ‘false alarm’; whereas in the general population it is ‘injury of head’.
The population health dashboard provides breakdown at local authority (LA) level and down to Medium Super Output Area (MSOA) level. This functionality will help provide insights as to the characteristics of the local population and their reasons for calling 999. These local insights will support localised decision making as well as identification of localised support needed. In the example provided in the Power BI example in this section, the age, sex and deprivation profile of the calls received within Burnley is compared to regional averages or to population figures as follows, in Burnley:
- The top reason for calls is illness and not falls or chest pain as across the region
- The number of calls from males, 15-19 years old, is considerably higher than the regional average (as denoted by the black marker along the respective age and sex bar)
- Deprivation index data indicates that 61% of the calls in Burnley come from locations in areas in the bottom 20% of deprivation, in contrast with an overall 32% of the population living in these areas.
In other areas of the trust, other actionable insights are being derived. For instance, Violence Prevention and Reduction reports have helped mapping trends to identify and implement interventions that aim to prevent offenders from re offending, and to provide support to the members of staff involved in such incidents. Interventions include reducing under-reporting of incidents, working alongside mental health, safeguarding teams and other partner agencies to assist in judicial outcomes, and/or trauma informed support to reduce re-offending. Finally, in relation to NWAS contribution to the evidence base on ambulance services working to support the reduction of health inequalities, NWAS staff collaborated in the publication of their work in academic journals, including an analysis to ascertain the prevalence and demographics of individuals who have died by suicide, and a retrospective analysis of care homes’ ambulance call-outs for seizures in North West England. https://pubmed.ncbi.nlm.nih.gov/32851820/
Public Health
Aligned to the trust vision ‘to provide the right care, at the right time, at the right place, every time’, the Public Health team continues working towards our aim to ‘work together to shape a better future’, working with patients, communities and partners to improve access, outcomes and experience for everyone, and helping to ensure patients get appropriate preventive care, not just an ambulance response, at times of need.
The population health and social value objectives in the Sustainability Strategy 2023-2026 outline how we will work together to improving health now, and for future generations by tackling health inequalities and focus upon prevention, by supporting improvement of the wider determinants of health in our communities. The deterioration of the health of our population, especially in the most disadvantaged groups, was highlighted in the Lord Darzi 2024 review. This places an emphasis on all health and social care providers to urgently focus on prevention, to reduce the current unprecedented levels of demand; we are committed to playing our part in addressing this through the engagement and delivery of our public health initiatives.
This year we have focused upon developing four key enabling foundations to support the trust in becoming an effective system partner to improve health and wellbeing, and to reduce health inequalities in our communities. Our public health workstreams are aligned to our objectives in the Sustainability Strategy and informed by policy and guidelines for NHS organisations. In relation to health inequalities included in the NHS’ Long Term Workforce Plan, is to ‘reform’ the NHS workforce and the NHS England statement on information on health inequalities, and the new government priority for the NHS, is to shift treatment to prevention. Utilising the output from our completion of the AACE Reducing Health Inequalities maturity matrix tool, the Public Health team has focused upon developing four enabling areas:
1. Building public health capacity and capability
2. Data, insight, evidence, and evaluation
3. Strategic leadership and accountability
4. System partnerships
Evidencing our commitment to this work, this year’s annual plan and Priority 3 of the EDI Plan included deliverables to improve our ability to reduce health inequalities for our population including our patients, members of the public and our staff.
Building Public Health Capacity and Capability
Baselining our current organisational position, regarding our public health capacity and capability, will provide us with a foundation to develop informed plans. Aligned to the Sustainability Strategy Deliverable PH06, we are conducting an analysis from a trust-wide Population Health Staff Survey to inform and develop future training plans. The survey generated 393 responses, received from across NWAS, including clinical and non-clinical staff as well as volunteers. The analysis and evaluation of the results, as well as informing the development of internal training plans, has the potential to inform the national position regarding public health capacity and capability in the ambulance sector.
Developing organisational and individual understanding of the opportunities each of us have to make a positive impact on health inequalities and how to act on them, is a key objective aligned to the NHS’ Long Term Workforce Plan, with the intention to ensure our workforce has the right skills and knowledge to shift care towards prevention and early intervention. The Public Health team, in collaboration with the Strategy and Learning and Organisational Development teams, has produced two introductory modules to increase awareness and understanding of health inequalities and to ‘make every contact count’. These modules will form part of the mandatory training cycle in 25/26. This work was supported by a small grant from NHS England North West’s Workforce Training and Education department and aligned to the Sustainability Strategy deliverable PH01.
We have reviewed and scoped opportunities to expand the public health specialist capacity within the organisation (Sustainability Strategy objective PH05). Through our engagement with the North West Public Health Workforce Matters Regional Forum, we were able to identify Level 6 Public Health Practitioner (PHP) Integrated Degree apprenticeship opportunities, and funding available to support employers with salary backfill, in addition to support from the apprenticeship levy. Via a structured application process, colleagues from both our paramedic emergency service (PES) and our patient transport service (PTS) are undertaking the programme, affording them the opportunity to both develop themselves professionally as well as developing public health knowledge and skills to apply in their own roles, contributing to improving population health.
Data: Insight, Evidence and Evaluation
Understanding where we see variation in access, experience, and outcomes for different population groups across NWAS services is a fundamental requirement, in order for us to target and deliver interventions to improve population health (Sustainability Strategy PH04). Working in collaboration with the Business Intelligence team, work was undertaken to develop a population health dashboard to provide demographic profile and relative demand of the population we serve to provide insights on health inequalities. This consists of a series of reports on 999 calls and incidents attended, broken down by patient characteristics (age, sex, and ethnicity), and by population health data (location and deprivation index). This information will be visible to all the trust and will help develop our understanding of differences in access and outcomes by patient groups. This will also help us identify the demand from our most vulnerable groups. This work aligns with the requirements from NHS England statement on information on health inequalities.
In addition, work was conducted by public health registrars on placement within the trust to undertake a preliminary analysis of PTS journeys between April 2022 – May 2023. They looked at characteristics of service users, as well as the demand by geographical areas. The analysis at LSOA level confirmed previous understanding of demand being driven by areas with higher proportion of population over 65 years, but some areas showed discrepancies with usage assumptions. The next steps are to validate the findings analysis and integrate them into a dashboard for PTS data which will then be incorporated into the public health dashboard.
We have also had conversations with research partners at the University of Liverpool to engage with their Masters of Public Health (MPH) and Masters in Data Science (MSc) programmes. This will look at collaborative opportunities to further analyse and evaluate our data surrounding public and population health. This work will continue and aligns to Sustainability Strategy Objective PH03 in developing relationships with research partners, to build the evidence base on the value of ambulance trust data and initiatives in prevention and tackling health inequalities.
Strategic Leadership and Accountability
The development of our public health workplan was undertaken following engagement with senior leaders, groups and committees, including the Public Health Oversight Group. It was based upon outputs of this consultation builds on our progress achieved in the previous three years, and outlines our intentions to ensure NWAS becomes an effective partner to improve health and wellbeing and to reduce health inequalities in our communities. Central to this are three core concepts:
- Developing solid foundations in organisational understanding of public health to enable the successful embedding of public health approaches across our working practices.
- Developing everyone’s understanding of the opportunities each of us have to make a positive impact on health inequalities and how to act on them.
- Developing our shared agreement of the top priority areas for prevention where we can make the most impact to population health across the North West.
We are confident that the public health workplan will directly inform and become part of the Strategy Development Programme to ensure a focus upon public health and health inequalities in all priorities across the trust, linking its objectives with our EDI objectives. within the strategy.
System Partnerships
We recognise our integral role in the wider health system and are striving to establish, develop and mature partnerships, particularly with ICS partners, to make best use of NWAS data and intelligence to inform system wide prevention initiatives (aligned to Sustainability Strategy PH03).
- Blood pressure data sharing. Leveraging ambulance data to improve hypertension management and prevent cardiovascular disease.
In England, hypertension is the number one risk factor for cardiovascular disease (CVD), mortality and morbidity. Poor CVD health can cause heart attacks, strokes, and other complications, with people living in the most deprived areas being more likely to suffer a stroke. Although estimates suggest that over one in three adults have hypertension, strikingly, over four in 10 adults with hypertension do not know they have this condition. Being aware of having hypertension is key to start lifestyle changes or treatment to keep this under control.
We continue to work with our GP partners to develop evidence to support a new data sharing pathway to share our data with them to help identify patients with undiagnosed or unmanaged hypertension. This year we completed a new pilot with a group of six GPs in Cheshire and Merseyside. This work is helping us demonstrate the potential for ambulance services to contribute meaningfully to preventative care, also helping to foster collaboration between NWAS, GPs, and other healthcare partners.
- Workplace health checks
In 2023, in collaboration with Liverpool Heart and Chest Hospital, the Public Health team and the Health and Wellbeing Team provided 45 cardiovascular disease health checks to staff as part of the Health and Wellbeing Festival in Liverpool. This year, thanks to engagement with partners across our Region, NWAS teams identified new opportunities to offer our staff health checks at the workplace, providing a total of 43 health checks at our base in Greater Manchester. This work is part of a national initiative from NHS England to support prevention of hypertension, heart disease, kidney disease, diabetes, and other diseases to our workforce. In addition, this year the Health and Wellbeing team worked with Liverpool Liver Unit to offer staff the opportunity to have a liver scan, with 40 scans provided.
- Sickle Cell Awareness Campaign
The Public Health team, working with the Race Equality Network, developed awareness materials to increase awareness within our population and workforce. This included information on the identification and prevalence of sickle cell, crisis and clinical management, health inequalities for sickle cell together with lived experiences
- Non-Fatal Drug Overdoses April 2025
The Public Health team has provided support and consultation to the trust’s overdose pathway practitioner to progress and define a referral pathway for our clinicians. An analysis of service provision identified no gaps in local authorities with service providers involved in the pathway. The pathway will be piloted over the coming year with a phased and gradually rolled out planned across the region.
Research and Development
We are extremely proud of the research work undertaken by the trust. Within NWAS, we have a wealth of experience and staff with first class clinical skills, who can influence change and educate others within the ambulance sector and the wider health system.
We develop, host, and deliver research that has a focus on pre-hospital urgent and emergency healthcare, injuries, and other clinical specialities. We also explore non-clinical research opportunities involving the organisation and our workforce. From clinical trials, looking at drug administration routes in patients with out –of hospital cardiac arrest, to research studies exploring staff views on clinical decision making when attending older adults who have fallen – NWAS actively contributes to the improvement of the care and experience of patients nationally, as well as within our own region.
The Research and Development (R&D) team strengthened partnerships with the National Institute for Health and Care Research (NIHR), health and care providers, higher education institutions and other external stakeholders to cultivate research collaborations. We continued to secure income from the NIHR to support the growth of our research infrastructure
We continue to increase the number of opportunities for patients, staff and the public to take part in the NIHR Research Delivery Network (RDN) Portfolio research studies across our organisation. During 24/25, 1,067 participants took part in high quality, national research, the highest ever participant recruitment to NIHR RDN Portfolio studies in our history. This was an increase of 53% over the last five years since 20/21.
Figure: NIHR RDN Portfolio Recruitment
Research activity continues to grow across the organisation. We act flexibly and strategically to maintain research capacity and capability, ensuring that we continue to strengthen the culture of evidence-based practice and can continue to deliver safe, effective, and patient-centred care.
Task Force on Climate Related Financial Disclosures (TFCD)
The DHSC Group Accounting Manual (GAM) has adopted a phased approach to incorporating the TCFD recommended disclosures as part of sustainability annual reporting requirements for NHS bodies, stemming from HM Treasury’s TCFD aligned disclosure guidance for public sector annual reports. TCFD recommended disclosures as interpreted and adapted for the public sector by the HM Treasury TCFD aligned disclosure application guidance, will be implemented in sustainability reporting requirements on a phased basis up to the 2025-26 financial year. Local NHS bodies are not required to disclose scope 1, 2 and 3 greenhouse gas emissions under TCFD requirements as these are computed nationally by NHS England.
The phased approach incorporates the disclosure requirements of the governance, risk management and metrics and targets pillars for 2024-25. These disclosures are provided below with appropriate cross referencing to relevant information elsewhere in the annual report and in other external publications.
Governance Pillar
The Sustainability Strategy 2023-2026 is one of four key underpinning strategies to achieve our vision and aims. Our Green Plan was developed in January 2022 and outlined how we plan to work towards Delivering a Net Zero NHS. A new three-year Green Plan is currently being developed in line with NHS England requirements, which will include mapped actions across all core themes specified within the Sustainability Report.
The Green Plan is overseen by the quarterly Sustainability Group and is chaired by the director of finance, who is the Board level sustainability lead and provides assurance that the trust:
- Complies with relevant legislation and guidance trust wide.
- Protects human health and the environment in relation to safe/proper environmental management.
- Takes an integrated approach to deliver services that efficiently use resources, finance, and infrastructure.
- Works to minimise the impact on the environment and embed sustainability into services, in line with the trust vision.
- Maximise the ability to improve health and wellbeing through the services provided.
- Enhances and develops relationships with staff, patients and wider stakeholders and embeds a sustainable culture across the organisation.
Assurance from the Sustainability Group is provided to the Trust Management Committee via an Escalation and Assurance report using the 3A format (Alert, Advise, Assure, including the key risks discussed/identified during the meeting).
The board of directors maintain oversight of climate related issues and the Green Plan through a bi-annual sustainability report presented to the Resources Committee and in turn, the chair of the Resources Committee submits written assurance of progress to the board of directors.
Risk Management Pillar
Emissions reduction and climate adaptation are mutually reinforcing essential aims to minimise the adverse effects on population health and health services. As an ambulance service, our resolve to adaptation is ever more essential, given the vulnerability of the population we serve. Despite rapid decarbonisation, global temperatures will continue to rise, and without adaptation, health impacts from heat, cold and flooding will worsen due to climate and sociodemographic changes.
The process for identifying, assessing and managing climate risk involves reviewing climate data, assessing local vulnerabilities, empowering the workforce, and allocating resources to reduce climate-related risks to health, healthcare infrastructure, and supply chains. Tackling this requires close collaboration across sectors – including industry, local authorities, the wider NHS, social care, and the communities we trust serve.
Our risk management process is live and dynamic, undertaken through regular risk assessments and evaluation processes. The Datix Cloud IQ (DCIQ) Enterprise Risk Management (ERM) system is used by the trust to record, manage and monitor risks throughout the organisation. The Annual Governance Statement provides details in relation to our risk management control framework and how risk is managed within our directorates of the Trust. As part of their remit, the Sustainability Group identify, assess and management climate related risks and review risks at each meeting.
Frameworks to support resilience in the health sector have been developed, and the plan for 25/26 is to build on this. We already make use of early warning systems as they play a crucial role in preparing us for the impacts of extreme weather, by providing timely alerts that allow for preventive measures. This also allows health impacts related to extreme weather events, monitoring health outcomes like syndromic trends during heatwaves, cold spells, or floods to be monitored.
Plan for Next Year
- Use clearer signposting of existing data and user-friendly training to help public health, contingency planning and sustainability teams make evidence-based decisions (to cross-reference rather than duplicate).
- Address aspects of climate change through new reports and guidance (such as the fourth Health and climate adaptation report)
- Prepare a specific climate risk register, considering climate-related risks to the whole trust and our operations.
Metrics and Target Pillar
Within NWAS, there is an emphasis on considering climate risks when making infrastructure decisions and designing new facilities, including enhancements like improved green spaces, drainage systems and passive cooling solutions. Climate change risk assessments identify the likelihood of current and future climate hazards and their potential impacts. This information helps improve understanding of required adaptation, and resilience-building measures as well as tracking impacts over time.
For 25/26 the Trust will start using the NHS England Climate Change Risk Assessment Tool (CCRA) to assess climate risks and provide a framework for adaptation that delivers consistent outputs for end-users to improve the adaptive capacity of our sites. This widely adopted tool provides a crucial step in building improved resilience to climate change and was developed through stakeholder engagement which enables the tool to be aligned with NHS needs and reflects current scientific knowledge for each climate hazard and impact.
The tool looks at organisational assets, such as buildings to assess the potential climate hazard against 6 categories (heatwaves, drought, cold weather, downpours and flooding, severe weather events and coastal flooding and erosion). Based on inputs, the tool will produce a current and future residual risk score (representing the remaining risk to our assets following the implementation of planned adaptations). The tool is to be used prior to recording a potential climate change risk on the Datix Cloud IQ (DCIQ) Enterprise Risk Management (ERM) system, as both qualitative and quantitative aspects of climate related issues are considered to determine which assets should be included in the sustainability reporting and disclosures 2025-26 onwards (based on their relevance and significance).
Annual Sustainability Report
Introduction
Following the ‘Delivering a Net Zero NHS’ report, all NHS trusts were asked to produce a strategy in the form of a Green Plan by January 2022, to outline how they plan to work towards Net Zero. Our latest Green Plan will be published by July 2025 and now includes mapped actions across all core themes, such as; workforce and system leadership, sustainable models of care, digital transformation, travel and transport, estates and facilities, medicines, supply chain and procurement, food and nutrition, and adaptation. The new Green Plan will cover a period of three years, 2025-2028.
24/25 has seen continued momentum for delivery of our net zero ambitions across NWAS, despite the ongoing pressures an ambulance trust faces. The Green Plan provides us with a framework to deliver sustainable emergency care and has complemented some of the innovations seen this year. Continued roll-out of initiatives such as electric vehicle charging infrastructure for rapid response vehicles and electrifying the estate for major capital projects, illustrates seized opportunities to scale-up decarbonisation initiatives, as well as build on those completed since a pause during the pandemic.
The following sections outline the progress we have already made in improving our carbon footprint and reducing the environmental impact of our services. It provides an overview of the NHS’ modelling and analytics, underpinning the carbon footprint, progress to net zero and the interventions made to achieve that ambition.
Energy and Water
Gas and electricity supplies have stabilised over the last 12 months as on a national level supply has diversified; more renewable energy capacity has been installed, and gas storage is now at an improved level. However, gas unit prices are still high since a 50% wholesale price increase in 2022. Gas costs increased by 11.5%, taking spending from £434,922 in 23/24 to £488,340 for 24/25, although conversely, electricity fell by 12.7%, taking spending from £1,872,518 last year to £1,648,518 for 24/25. This can be attributed to reduced tariff costs and continued roll-out of energy efficiency schemes.
Water costs have increased 13.1% due to supply point charge increases, taking spending from £315,938 in 23/24 to £360,364 this year.
Aim
Reduce carbon emissions from energy use, in line with data informed budgets to be on track for net zero by 2040:
- Use less energy
- Replace fossil fuels with low and zero carbon energy sources
- Investigate options to offset, or inset our residual carbon emissions
- Minimise water use in our buildings and eliminate wasted water
- Increase water efficiency
Performance
- Carbon emissions from building energy use increased marginally by 195 tonnes in 24/25, but is 4,929 tCO2e below the baseline year of 2013
- This 99.2% decrease is due to a reduction of fossil fuels, both directly (scope 1) and indirectly (scope 2 – decarbonisation of the grid)
- Overall gas use for space heating increased slightly due to colder snaps during winter and the last oil-fired boiler in the Trust was decommissioned and replaced with an air source heat pump
- Overall electricity demand has decreased by 9.9%, due to staff homeworking and the continued roll-out of energy efficiency schemes, such as LED lighting across the estate
- However, demand for electricity is likely to increase at most of our sites in the coming years, mostly attributable to further use of heat pump technology to degasify the estate
| Utility | Carbon emissions (tonnes) | Consumption (kWh) | Gross Cost (£) |
| Gas | 1,406 | 7,594,212 | 488,340 |
| Electricity | 1,096 | 4,614,888 | 1,648,518 |
| Total | 2,502 | 12,209,100 | 2,136,858 |
Table: Utility usage and costs 24/25
Figure: Carbon Emissions – Energy Use
The trust continues to move in the right direction in line with the annual reduction pathway towards net zero by 2040.
| Utility | Consumption (m3) | Gross Cost (£) |
| Water | 35,791 | 360,634 |
Table: Annual reduction pathway towards net zero
Figure: NWAS Carbon Emissions – Water
- Carbon emissions from water use and treatment have increased by 8.6% in 24/25 compared to the previous year. This is due to a small increase in consumption, but the trend is still heading in the right direction thanks to revised carbon conversion factors (published nationally) and applied to actual consumption data for our sites.
- Although mains water consumption can vary year –on year, the general direction is making progress to net zero. In 2013, the trust consumed 42,677m3 of water, whereas for 24/25 total consumption was 35,791m3.
We are going into 25/26 more informed than ever before, following several completed feasibility studies and on-going works. These include:
- Deep dive energy surveying by the sustainability team at eight of our sites, identifying projects which could bring about carbon savings of over 400 tonnes per annum.
- Feasibility studies around fuel cell CHP, heat batteries and VRV/VRF systems and their wider use.
- Building fabric assessments using our in-house developed heat loss calculator.
- New electricity connection upgrades for seven of our sites to enable electrification of the buildings (and vehicles), with a further three in planning and rest of our sites at feasibility stage.
- Finalising works to enable Glossop and Winsford ambulance stations to become the official first net-zero ambulance stations within NWAS.
Work with other blue light services, city and regional partners has increased, particularly around progressing a feasibility study for a heat network at co-located sites in Greater Manchester, (this work also extends to EV charging mentioned in later sections). This has culminated in a more strategic estates decarbonisation group, which will play a key role in steering the transformational change required to deliver these ambitious carbon reduction objectives.
Given the energy market, we are in a reasonable position with prices protected for the forthcoming financial year to remain on a 100% zero carbon energy tariff. This was only achieved through a combination of reducing payment terms, further digitising billing, and eliminating unnecessary standing charges.
Plans for Next Year
- Prioritise decarbonisation projects based on the learning from the feasibility studies outlined above
- Agree an LED rollout programme which builds on existing works to achieve 95% or more coverage by end of 2026
- Improve energy optimisation through Building Management System (BMS) projects and management practices
- Deliver projects for solar and battery storage for 11 sites using funds secured form the Department of Energy Security and Net Zero and NHS England.
- Continue to develop and feed-in decarbonisation investment opportunities for the estates capital programme
- Further infrastructure and decarbonisation feasibility studies including connection upgrades, solar PV feasibility assessments and alternative heat technologies
- Investigate the potential for innovative zero carbon procurement options such as power purchase agreements (PPAs)
- Continue to explore options for modular buildings to assist in the estate reaching net zero.
- Improve engagement on decarbonising the estate both within the Estates directorate and trust wide
Despite the demands from our buildings and estate, the plan for the forthcoming year is to drive energy reductions and use resources as efficiently as possible.
Waste
Aim
- Generate less waste; reuse and recycle more, and ensure unavoidable waste is disposed of in the most sustainable way
- Reduce the amount of waste we create by working and purchasing in more resource efficient ways
- Increase the number of items we reuse with a focus on reducing single use plastics.
- Repair or reuse more items that can be repaired or reused
- Increase the amount of waste that we reuse or recycle to 50% of consignment waste by volume, which NWAS were on the way to achieving pre-pandemic.
- Maintain zero waste to landfill
Figure: Annual Waste Performance (overall tonnage and percentage by waste outcome)
Performance
Clinical Waste:
As we continue to respond to the pandemic, clinical waste volumes increased in line with the demands involved with higher patient activity. Since then, we have actively been winding-back additional collections and reclassifying clinical wastes to reduce tonnages to pre-covid levels. Further work is planned for 25/26, which will see large portions of waste destined for high temperature incineration, disposed of through alternative treatment and offensive waste streams, meaning the carbon footprint (and associated costs) will be reduced as we strive towards NHS England’s 20:20:60 split for clinical waste target. NHS England encourages a split of 60% offensive waste, 20% waste sent for high temperature incineration (HTI), and 20% of waste sent for alternative treatment (AT). If successful, this would reduce our high temperature incinerated waste to <10% of current tonnage. We are also part of a working group exploring options to dispose of clinical waste at hospital sites as part of a pilot with NHS England. This would represent a huge efficiency saving to ambulance trusts and go way beyond the 20:20:60 target.
General and Workshop Waste:
General waste volumes have remained consistent for the last few years (except for 20/21) and as a result there have been no significant changes in waste composition or total waste volumes. We continue to ensure that all recyclable material, such as paper, cardboard, plastics, metals and glass are segregated at the point of generation, and that all provisions are in place for hazardous wastes such as used engine oils, other engine fluids and batteries for safe disposal.
Plans for the Next Year
- Examine the disposal routes for all materials across the trust and look to move waste up the waste hierarchy
- Work with colleagues in Procurement and the NHS Supply Chain for a deeper investigation into data related to key product categories of single use plastic – aimed at reducing consumption
- Collaborating with ICBs to look at waste management and proposals for a regional approach to reuse and recycling
- Staff training and understanding will be improved by embedding the healthcare waste management guide into local inductions, and developing additional waste training (such as toolbox talks, IPC linked ESR training and guidance documents)
- To develop a metric for measuring and reporting of reuse
Fleet, Travel and Logistics
The trust produces significant carbon emissions from fleet, staff travel, and the logistics associated with our activities and service provision. To deliver high quality care, we make use of a large and varied fleet of vehicles, and the analysis accounts for all vehicles used for NHS duties that are directly owned and leased by the trust with emissions totalling approximately 8,223 tCO2e for 24/25.
We aim to ensure all vehicles purchased or leased are low and ultra-low emission (ULEV), in line with existing NHS operating planning and contracting guidance, and that they meet the NHS Long Term Plan commitment for 90% of the NHS fleet to use low, ultra-low and zero emission vehicles by 2028. Ambulances pose a specific challenge and require targeted interventions, but for the rest of the fleet, we continue to explore options for a complete transition to zero emission vehicles by 2032.
Aim
- To embed active, clean and low carbon travel to improve air quality and reduce carbon emissions from journeys
- Reduce air pollution and carbon emissions from our owned and commissioned transport operations
- Use our influence to help fast-track the decarbonisation of transport in our supply chain
- Increase the proportion of people commuting to our sites using active and sustainable travel methods
Performance
- This year we have seen a 3.3% increase in vehicle miles, and subsequent increase in emissions of 115 tonnes stemming from increased mileage from PES vehicles
- Despite the increase in vehicle miles, there has been a 13.1% reduction in emissions compared to the baseline year of 2013. A significant proportion of this decrease is linked to a reduction in business travel since the pandemic, efficiency improvements in diesel vehicles and the aforementioned roll out of electric service vehicles
- There has also been a significant increase in the number of staff using electric vehicles and hybrids due to emission limitations impose for business fleet vehicles
- There has been active links with transport authorities to enable more incentivised travel for staff in more urbanised areas. This also links to the planned review of all trust sites to ensure they are accessible by public transport and that active travel facilities are provided on all trust sites, such as secure cycle parking, showers and lockers
- Our Car Lease Policy has also undergone review to promote the use of low carbon and zero emission vehicles to essential users within the trust
Carbon Footprint
The information provided in the previous versions of this annual report uses the ERIC returns as its data source. However, we are aware that this does not reflect our entire carbon footprint. Therefore, the following information estimates the impact of our supply chain from our spend.
Figure: Proportions of Carbon Footprint
Resulting in an estimated total carbon footprint of 23,806 tonnes of carbon dioxide equivalent emissions (tCOâ‚‚e).
The Accountability Report
Our Accountability Report has been prepared to meet key accountability requirements to parliament and is based on matters required to be dealt with in a Directors’ Report, as set out in Chapter 5 of Part 15 of the Companies Act 2006 and Schedule 7 of SI 2008 No 410, The Large and Medium-sized Companies and Groups (Accounts and Reports) Regulations 2008, and in a Remuneration Report, as set out in Chapter 6 of the Companies Act 2006 and Schedule 8 of SI 2013 No 1981, The Large and Medium-sized Companies and Groups (Accounts and Reports) (Amendment) Regulations 2013.
Salman Desai KAM Date: 18 June 2025
Chief Executive
Corporate Governance Report
Directors’ Report
Board Membership
In accordance with the Membership and Procedure Regulations 1990 (as amended) Trust’s Standing Orders, the NWAS Board of Directors comprised of a non-executive chair, five non-executive directors, seven executive directors; five voting and two non-voting. The board of directors is a unitary board and has a wide range of skills and experience. Non-executives have wide-ranging expertise and experience including backgrounds in finance, internal audit, primary care, education, health and social care and HR.
Non-executive Directors
Peter White, Chair
Peter joined the trust as a non-executive director in 2014 and acted as vice chair, with specific responsibility for performance and quality, as well as leading on behalf of the board on EPRR (Emergency Preparedness, Resilience and Response). Peter also served as a non-executive director in a national housing association and chaired their neighbourhood services committee. He is also deputy chair of a community interest company who deliver adult social care in Oldham. Peter has used his experience to support the organisation in developing its governance and performance management processes. Prior to these roles, Peter enjoyed a varied career, policing all areas of Lancashire from 1983 until his retirement in 2013.
Peter has been a public servant for over 40 years and has a strong service ethos, whether as a senior police officer or a non-executive director he is motivated by supporting organisations to provide the best possible services to the public.
Catherine Butterworth, Non-Executive Director
Cathy was appointed non-executive director on 1 April 2022 and is the trust’s Wellbeing Guardian. She also holds a non-executive director position for three health and social care companies in Oldham and is currently operating as interim chair of MioCare Board. Cathy has held numerous HR roles for both Greater Manchester Police and the British Transport Police, and was assistant director of people for Oldham Council from 2012-2018. A HR consultant for various NHS organisations, Cathy has delivered workforce strategy and planning aspects of HR and has contributed to transformational change across organisations and their partners, including the integration of health and social care at regional and borough levels.
Alison Chambers, Non-Executive Director
Alison was appointed non-executive director on 1 August 2019 and is the senior independent director and vice chair. She also holds the position of non-executive director and senior independent director at Pennine Care NHS Foundation Trust. Alison is also a trustee with Pendle Education Trust, with lead responsibilities for special education needs. She has a significant and successful track record of strategic partnership development, large scale organisational change management, strategy development, implementation, and delivery. Alison qualified as a chartered physiotherapist in 1985 and worked in clinical practice for 10 years before moving into higher education. Her academic roles include pro vice chancellor at Manchester Metropolitan University and Professor of Healthcare Education.
Aneez Esmail, Non-Executive Director
Aneez joined the trust on 1 April 2021 as non-executive director and is currently chair of the Quality and Performance Committee. Esmail is Emeritus Professor of General Practice at the University of Manchester. He has experience as a researcher, teacher, and clinician. His research interests are focused on patient safety, burnout in healthcare professionals, inequalities in health, the organisation and delivery of health services and public health. He has published over 100 academic papers in these areas. He worked as the medical advisor to the appeal court judge who chaired the Shipman Inquiry between 2001-2005, and played a key role in developing the recommendations that resulted in significant changes on the reform of the General Medical Council, death certification and investigation, controlled drugs regulation and the regulation and revalidation of doctors.
He was commended by the Health Service Journal, as one of the top 100 clinical leaders in the NHS in 2014 and received the Lifetime Award for Achievement in General Practice in 2017 from the publishers of Pulse Magazine. He also received a Medal of Honour from the University of Manchester in 2023 for his contributions to public health, his challenges to racism in the medical profession and his significant contributions to the senior leadership of the university.
David Hanley, Non-Executive Director
David was appointed non-executive director on 28 May 2019 and is chair of the Resources Committee. He has worked at a senior level in health and social care for 30 years. During this time, he oversaw significant service development and change, as well as managing large staff groups, annual budgets in excess of £50 million, and challenging service environments. Leading on partnership working, particularly with health services. David studied for a PhD in his spare time and left his management role to pursue an academic career, firstly at Bolton University, and then at UCLan, however retired from the University in 2023.
David Whatley, Non-Executive Director
David joined as associate non-executive director (audit chair designate) on 1 April 2023 and was appointed non-executive director and audit chair on 25 March 2024. His accountancy career began as an auditor at Pendle Borough Council and he has held senior roles in GIAA, including group chief internal auditor for a range of departments and head of internal audit for several arms length bodies. GIAA was set up as an executive agency of HM Treasury in 2015 to improve the quality of internal audit provided to central government, delivering internal audit services to a number of departments and associated bodies.
David is a member of the Chartered Institute of Public Finance and Accountancy and achieved the Diploma Management Studies and is accredited as a local counter fraud specialist (LCFS). Previous roles have included being head of audit at the Health and Safety Executive (HSE) and a director at RSM Bentley Jennison.
Executive Directors
Daren Mochrie, Chief Executive QAM (left 30 November 2024)
Daren joined NWAS as Chief Executive in April 2019 and is also chair of the Association of Ambulance Chief Executives; a membership body for all UK ambulance services and Crown Overseas Territories. He has over 35 years’ experience in the NHS, with 32 years in the ambulance sector and is a registered paramedic. Daren holds a Master’s degree in Business Administration from Napier University, a Diploma in Immediate Medical Care from the Royal College of Surgeons, and an Honorary Doctorate in Health Care.
Daren has been an inspection chair and specialist advisor with the Care Quality Commission, and trustee of an air ambulance charity. He has also worked in a number of UK ambulance services at executive director/ CEO level. He has led transformational change in several ambulance services and improved their CQC ratings and continues to champion nationally the voice of the ambulance sector. Daren was Chair of AACE from August 2020until August 2024 and during this time, led the sector through the COVID- 19 pandemic, the most challenging winter in the NHS in 2022 and industrial action. In 2013, he was awarded the Queens Ambulance Medal for distinguished service.
Salman Desai, Chief Executive KAM (from 1 January 2025)
Acting Chief Executive (July 2024 to 30 December 2024)
Deputy Chief Executive/Director of Strategy, Partnerships and Integration (to 30 June 2024)
Salman was appointed chief executive on 1January 2025 following a period as the trust’s acting chief executive. Salman has over 25 years of service in the NHS, initially training as a paramedic, a registration he still holds today, before moving into other roles. He has worked across various sectors covering the ambulance service, acute sector, and wider public sector where his work focused on preventing death from drug use among marginalised communities in Greater Manchester. More recently, he has been the chief operating officer and leading on strategic planning, transformation of trust resilience following the pandemic and developing a partnership and integration function that will help with influencing and working more effectively across the multiple systems and places we serve. He joined the board of directors in 2015 as associate director of strategy and planning.
Dan Ainsworth, Executive Director of Operations (from 1 July 2024)
Dan is Director of Operations at North West Ambulance Service. He has 16 years of NHS service with the past 11 being with NWAS. He has an educational background in law and holds a Law Degree (LLB) from the University of Sheffield. He has worked within a number of roles within the NHS and NWAS. Prior to joining the NHS, he worked with the pharmaceutical and publishing sectors. He initially commenced his NHS career as a health advisor for NHS Direct. He worked at all management levels within the NHS 111 service, then moved into the role of strategic head of EOCs for NWAS. More recently, Dan held the post of integrated contact centre director. He has significant experience working at the national level, representing the ambulance sector, chairing the National Heads of EOC Group for three years and this year has been nominated as deputy chair of the National Director of Operations Group. He has represented the sector in a range of national service change and transformation programmes. Dan’s focus is delivering high quality performance and patient care, empowering and developing leaders and enhancing the culture within the ambulance service.
Dr Chris Grant, Executive Medical Director
Chris is the Executive Medical Director at North West Ambulance Service NHS Trust. He has board responsibility for all the clinical elements of NWAS services and provides professional leadership for the healthcare professionals in the service. He acts as the Caldicott guardian, controlled drugs accountable officer, research and development lead, public health and health inequalities lead and is also responsible for the air ambulance. He completed his undergraduate training at Kings College London, before continuing his post graduate training in hospitals across the North West and subsequently in both Australian and the United States.
Dr Elaine Strachan-Hall, Interim Executive Director of Quality (commenced 17March 2025)
Elaine is an experienced clinical leader with over 45 years of healthcare experience, 20 years of which have been at board or director level, invariably holding the governance and quality portfolio in addition to professional leadership. Since COVID, Elaine has worked in a consultancy capacity assisting NHS trusts with large scale improvement programmes and individual ‘test of change’ projects. As a registered nurse who has recently completed her doctorate in nursing, she has a special interest in digital innovation and strategic nursing leadership. Elaine has stepped in to support NWAS in the role of interim executive director of quality, with responsibility for patient safety, innovation, and improvement.
Maxine Power, Executive Director of Quality, Innovation, and Improvement (left 31 March 2025)
Maxine is an NHS executive and improvement leader with over 30 years’ experience leading improvement. Initially trained as a clinician, Maxine has had an eclectic career working across clinical practice and academia in a variety of settings. Maxine has over 20 peer reviewed publications in improvement focussing on large scale change, measurement, evaluation, and patient safety. Maxine is the Executive Director of Quality, Innovation, and Improvement at the North West Ambulance service, with responsibility for patient safety, innovation, improvement, and digital systems. Her work involves leadership across four integrated care boards in the North West and she presents nationally and internationally on systems leadership for quality, safety, improvement and digital.
Lisa Ward KAM, Executive Director of People
Lisa has held the role of Director of People since July 2018, initially in an interim position until taking up the role permanently in 2020. Prior to this Lisa had extensive experience in senior human resources leadership roles in NWAS and its predecessor organisation Greater Manchester Ambulance Service. Prior to joining the ambulance service, Lisa spent 10 years in human resources management roles in the Midlands and North West working for the rail industry, having joined as a graduate management trainee following graduation with a degree in history from the University of East Anglia.
Lisa is a Chartered Member of the Chartered Institute of Personnel and Development (CIPD) and has undertaken a range of continuing professional development, including management, coaching and psychometric testing qualifications during her career.
Lisa was recognised in the 2024 King’s New Year Honours and awarded the prestigious King’s Ambulance Medal.
Angela Wetton, Executive Director of Corporate Affairs
Angela joined the trust as Director of Corporate Affairs, a non-voting board role, in September 2016. She has over 15 years board and sub-board level experience in corporate affairs, governance, and risk across public and private sectors. She graduated from the Nye Bevan Leading Healthcare Programme in April 2016 with an Executive Leadership in Healthcare award and prior to NWAS, had worked at Warrington and Halton Hospitals NHS FT, Calderstones Partnership FT, Lancashire Care FT, and Wirral University Teaching Hospitals FT.
Carolyn Wood, Executive Director of Finance
Carolyn is a Chartered Public Finance accountant and joined the trust as the executive director of finance in April 2019, having previously held the post of director of finance at Oldham Care Organisation, part of the Northern Care Alliance. She brings with her nearly 30 years of experience in NHS finance, having worked for a range of NHS organisations across the North West including Salford Royal, Royal Bolton Hospital, Cumbria PCT, North West Strategic Health Authority, NHS England (Lancashire), and Wrightington, Wigan and Leigh NHS Foundation Trust.
Attendance of Board of Directors Meetings and Committees during 24/25:
| Board Member | Term of Appointment | Board of Directors | Audit Committee | Nominations & Remuneration Committee | Charitable Funds Committee | Quality & Performance Committee | Resources Committee |
| Attendance (actual/max) | |||||||
| Non-Executive Directors | |||||||
| Peter White (Chair) | 1/2/19 – 1/2/23 1/2/23 – 31/1/25 1/2/25 – 31/7/25 | 8/8 | 7/7 | ||||
| David Hanley | 28/5/19 – 27/5/21 28/5/21 – 27/5/23 28/5/23 – 27/5/25 | 7/8 | 5/7 | 2/4 | 5/6 | 5/5 | |
| Alison Chambers | 1/8/19 – 31/7/21 1/8/21 – 31/7/23 1/8/23 – 1/8/25 | 7/8 | 5/6 | 5/7 | 5/6 | ||
| Aneez Esmail | 1/4/2021 – 31/3/23 1/4/23 – 31/3/26 | 6/8 | 5/6 | 5/7 | 6/6 | ||
| Catherine Butterworth | 1/4/22 – 31/3/24 1/4/24 – 31/3/26 | 7/8 | 6/6 | 4/7 | 4/4 | 4/5 | |
| David Whatley | 24/3/24 – 24/3/26 | 8/8 | 6/6 | 7/7 | 4/4 | 5/5 | |
| Executive Directors | |||||||
| Daren Mochrie | Left 30/11/24 | 4/6 | |||||
| Chris Grant | 6/8 | 5/6 | |||||
| Salman Desai | 8/8 | 3/3 | 2/2 | 3/3 | |||
| Dan Ainsworth | Commenced 1/7/24 | 4/5 | 2/3 | 4/4 | 4/4 | ||
| Angela Wetton | 6/8 | 3/4 | 6/6 | ||||
| Maxine Power | Left 31/3/25 | 8/8 | 5/6 | ||||
| Lisa Ward | 8/8 | 2/4 | 4/5 | ||||
| Carolyn Wood | 8/8 | 4/4 | 5/5 | ||||
| Elaine Strachan-Hall | Commenced 17/3/25 | 1/1 | |||||
Committees
A number of assurance committees reported to the board of directors during 1April 2024 and 31 March 2025, these committees were as follows:
Following a review of the governance structure during Q4 of 23/24, a new governance framework was established from 1 April 2024. The Annual Governance Statement (AGS) describes the aims of the review.
Each committee has formal terms of reference which are approved by the board of directors and sets out the powers and functions of the committees. These terms of reference are subject to annual review by the relevant committee with outcomes subsequently reported to the board of directors for approval. This annual review process incorporates a review of committee effectiveness against five themes and identifies areas of development to further strengthen their remit. The five themes committees are assessed against are:
- Committee focus
- Committee engagement
- Teamworking
- Effectiveness
- Leadership
Following the annual review, the committee chairs for the Quality and Performance Committee and Resources Committee submit an annual report to the board of directors providing information on how the committee met its key functions during the year and key areas of focus for the following year. The terms of reference for all committees are reviewed on an annual basis and approved by the board.
Audit Committee
The terms of reference for the Audit Committee are based on the model terms of reference incorporated in the HFMA Audit Committee Handbook.
During Q1 24/25, the committee carried out a review of its effectiveness against the two checklists provided within the HFMA Audit Committee handbook to 1) testing the committee processes and 2) to test its effectiveness against a number of themes; focus, team working, effectiveness, engagement and leadership. Whilst the outcome was positive, there were a small number of areas that required review with executive leads in relation to checklist two and was addressed through an action plan developed by the chair of the committee and presented to the committee on 18 October 2024. Members of the Audit Committee held private meetings with internal and external auditors during the year.
Members of the Audit Committee during 24/25 were David Whatley (Chair), Alison Chambers, Aneez Esmail, and Catherine Butterworth. The chair of the committee has the relevant financial experience. The chair of the Audit Committee, David Whatley presented the Annual Report of the Audit Committee to the NWAS Board of Directors on 30 April 2025 which provided a summary of the activities undertaken by the committee and how the terms of reference and key priorities were met during 24/25. The Audit Committee terms of reference for 25/26 were updated in accordance with the HFMA Audit Committee Handbook and approved by the board on 30 April 2025.
In April 2025, the Audit Committee received an update relating to the trust’s compliance against the NHS Provider Code of Governance during 24/25. The NHS Code is based on the UK Code of Governance to reflect latest and best practice application of good corporate governance and provides a tried and tested framework for the leadership and direction of board led organisations in the UK. A summary of the trust’s corporate governance arrangements against the NHS Code was provided to the committee for assurance and the trust was able to declare compliance with all relevant provisions.
The Audit Committee is charged with oversight of the trust’s compliance with the NHS Provider Licence. The committee received the annual declaration of compliance with the conditions of our NHS Provider Licence during 24/25 at its meeting in April 2025.
A key aspect of the Audit Committee is to consider significant issues in relation to financial statements. As part of the preparation for the audit of financial statements, Forvis Mazars undertook a risk assessment and identified the significant risks as management override of controls, risk of fraud in expenditure recognition – all of which are required under the auditing standards. In addition, significant risks related to valuation of property, plant and equipment were considered, the Audit Committee did not raise any specific issues in relation to these areas.
External Auditors
Following recommendation from the Audit Panel, the Board of Directors approved the contract award from 1 April 2024 for a period of two years with the option to extend for two further 12 month periods to Forvis Mazars LLP.
The audit fee for the 24/25 financial statements is £100,000. Forvis Mazars LLP have not provided the trust with any non-audit services during the reporting period.
The outcome of a formal assessment into the effectiveness of external audit was received by the Audit Committee in January 2023 and indicated a high level of satisfaction in the work undertaken by the external auditors. Formal assessments have been scheduled to be undertaken every three years.
During 24/25, the Financial Reporting Council (FRC) carried out an Audit Quality Review Inspection on the external auditors work on the Trust’s 23/24 financial statements and value for money arrangements. FRC found no significant improvements were required.
Internal Audit
Internal audit and anti-fraud services are provided by Mersey Internal Audit Agency (MIAA).
Independence of Directors
All directors have a responsibility to declare relevant interests as defined within the Board Standing Orders and Standards of Business Conduct. The trust maintains a Register of Interest for the NWAS Board of Directors and is subject to bi-monthly review by the board. Where details of company directorships have been declared and where those companies are likely to do business or are seeking to do business with the NHS, board members declare their interest and withdraw from any decision making process. During 24/25, there were no identified breaches in respect of any declarations made by the board of directors.
All non-executive directors are considered to the independent and provide independent scrutiny and challenge to the board.
The board of directors register of interest is available to view here.
Statement of Disclosure to Auditors and Directors’ Responsibilities
It is the responsibility of directors to prepare the annual report and accounts. They consider the annual report and accounts, taken as a whole, is fair, balanced, and understandable, and provides the information necessary for stakeholders to assess the trust’s performance, business model and strategy.
As far as the executive directors are aware, there is no information relevant to the auditors for the purposes of their audit report. The executive directors have taken all of the steps they ought to have taken to ensure they are aware of any relevant audit information and to establish that the auditors are aware of that information.
Fit and Proper Persons Requirements: Directors and Non-executive Directors
In line with the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014, the trust is required to ensure that all individuals appointed to or holding the role of executive director (or equivalent) or non-executive director meet the requirements of the Fit and Proper Persons Test (Regulation 5) and the additional checks set out in the Fit and Proper Persons Test framework.
The trust has fully implemented the requirements of the Fit and Proper Persons test framework, including social media checks, DBS checks, annual attestation, inclusion of board level competences in appraisal, appropriate pre-employment checks and board references. In line with the requirements of the framework, the chair signed the completion of a Fit and Proper Person assessment for all individual board members to the relevant NHSE regional director. This included confirmation of a satisfactory appraisal from the preceding 12 months for all board members.
In May 2024, the board of directors received the chair’s annual declaration confirming that all existing executive and non-executive directors met the requirements of Fit and Proper Persons Test which was informed by the application of the board approved procedure on fit and proper persons requirements.
An annual audit of the personal files has been undertaken to ensure that the files remain up to date and in line with the regulations.
An independent internal audit of fit and proper persons procedures and records was undertaken in June 2024. This provided high assurance and included no recommendations
Well-Led
Following a procurement exercise, Deloitte LLP carried out an externally facilitated developmental review of leadership and governance in 19/20. Whilst there were no areas of major concern, 19 recommendations were provided to further enhance governance and leadership arrangements within the trust. An update was provided to the board of directors in December 2020, with full completion of actions in 22/23. Deloitte LLP had no connection with the trust nor any individual directors.
During Q4 24/25, a procurement exercise commenced to carry out an externally facilitated review of governance and leadership to commence Q1 25/26.
Information Governance
Information Governance work programme throughout 24/25 has been reported to the Information and Cyber Group, (ICG), chaired by the senior information risk officer (SIRO). The ICG reports to the trust management committee through an assurance report. ICG effectiveness is monitored via the annual governance process.
The work programme aligns to the assertions set out in the Data Security and Protection Clinical Toolkit (DSPT). A focus on the work programme in year has been the management of information assets, including developing the information asset register, identifying and training information asset owners (IAOs) and information asset administrators (IAAs), cyber security, and data quality.
We have a well-established team with the trusts Data Protection Officer (DPO) provided by a third party, and the trust cyber security lead well integrated with the team.
Key areas of delivery and assurance are outlined as follows:
- Board Assurance: The Board Assurance Framework (BAF) included a strategic risk pertaining to cyber security, which provided the opportunity for escalation of risk and assurances to the board of directors on a quarterly basis.
- Policies and Procedures: There is a continuous review of policies managed and overseen by the ICG, with this year seeing a refresh to the Clinical Information Records Policy and CCTV Policy and the introduction of the Clinical Imagery Policy.
- Data Security Protection Toolkit (DSPT) 2024: The submission of the DSPT for 23/24 was on 27 June 2024. The trust submitted a score of 111 of 113 mandatory evidence. Two assertions were not met for which an improvement plan was submitted for these assertions. This gave the status of the final submission ‘standards not met’. The improvement plan was reviewed by NHS England and the status was changed to ‘approaching standards’. Mersey Internal Audit Agency gave the trust substantial assurance.
- DSPT 2025: The DSPT was updated to reflect health care amended cyber assurance framework (CAF), it is still to be known as the DSPT. The updated DSPT provides a systematic and comprehensive approach to assessing the extent to which cyber and information governance risks to essential functions are being managed. The final submission deadline is 30 June 2025, the trust submitted an interim position on 31 December 2024. The interim submission showed of the 47 outcomes, 14 did not meet the required standard. An improvement plan is in place to close the gap but it is expected that not all standards will be met in 24/25.
- Data Breaches: During 24/25 financial year, 157 breaches relating to information governance were reported. Each information breach is risk scored against the trust’s risk matrix and investigated thoroughly. Level 4-5 breaches (most serious) are reviewed by the Information Governance team to determine whether they meet the criteria for referral to the Information Commissioners Office. Five incidents were reported, after meeting the criteria for notification to the ICO, with no action taken against the trust on two of the breaches and we are awaiting the outcome for the other three breaches. Learning from information incidents and breeches is discussed at Information Governance team level and escalated to the Information and Cyber Group. Action plans are developed for management of local issues and sharing of learning.
- DPO Complaints: The data protection officer (DPO) received a total of eight complaints (due to staff absence and the required deadline such figures do not include Q4). All complaints have been escalated, reviewed and closed.
- Data Protection Impact Assessments (DPIAs): Strong processes are in place to enable delivery of Data Protection Impact Assessments (DPIAs). Five full DPIAs have been completed for new and existing assets.
- Trust ID
- Induction and onboarding automation
- TP health
- Troponin Project
- DCIQ Phase 2
- Aspirer
- Data Sharing Agreements (DSAs): 11 information sharing agreements have been completed:
- Medical Examiners System Access Agreement
- Lancashire Resilience Forum Preparing for Emergencies update
- NWAS/Wirral University Health Trust (WUTH) review patients conveyed to WUTH who are discharged without treatment
- Tameside Adults Safeguarding Partnership Board and Tameside Safeguarding Children Partnership between Partner Agencies à Tameside Safeguarding Children Partnership, NHS Greater Manchester and Greater Manchester Police
- MFT NHS FT Troponin project
- Stockport NHS FT Serum Troponin project
- Haydock and Newton PCN hypertension management
- NWAS/Office for Health Improvement and Disparities – opiate o/d data sharing
- Tameside and Glossop Integrated Care NHS FT – cardiac care improvement
- North West Air Ambulance re PaNDA (Paediatric and Neonatal Database of Airway Management)
- North West main review of HEMS Base
- Subject Access Requests (SARs): Our Individual Rights team has received subject access requests (SARs), access to health requests, and numerous redirections of requests across the trust. A total of 3,147 requests (including SARs, access to health requests, and redirections) came into the trust between April 2024 and March 2025
- SIRO Key Performance Indicators: All key performance indictors (KPI) for freedom of information requests, subject access requests, data protection requests and externally reportable data breaches (within 72-hour timeframe) were met.
| KPI | Target | Q1 | Q2 | Q3 | Q4 | Overall |
| Freedom of information requests (FOI) | To respond to 90% of requests within 20 working days. | 99.16% | 100% | 100% | 100% | 99.79% |
| Subject access requests (SARs) | To respond to 85% of requests without undue delay and at the latest, within one month. | 99.59% | 100% | 99.62% | 99.60% | 99.67% |
| Data protection Requests | To respond to 85% of requests within 40 working days | 100% | 100% | 100% | 100% | 100% |
| Data breaches | To report any externally reportable data breaches within the 72-hour timescale. | 100% (0) | 100% (1) | 100% (1) | 100% (3) | 100% (5) |
Modern Slavery Act 2015
In order to support Integrated Care Boards and providers, NHS England (NHSE) has drafted a Modern Slavery Statement as a ‘group statement’ for NHS organisations to refer to, to reduce administrative burden, prevent duplication and increase consistency with organisations strongly encouraged to defer to this ‘group statement’. The statement covers the actions taken by NHSE to support the wider NHS to address the risk of modern slavery in the health service and point to actions best delivered nationally and locally.
The statement can be found by following the link below:
External Compliance
The trust’s functions are organised to ensure effective compliance with the external requirements placed upon it by bodies such as the Department of Health and Social Care, the Care Quality Commission, NHS England, and NHS Resolution. The trust aims to comply with, and meet, all statutory, legislative, and regulatory requirements placed upon it as an employer, an ambulance service, and an NHS trust. These include:
- National targets for ambulance response times
- Statutory and regulatory financial duties
- Care Quality Commission registration requirements
- NHS Model Employer standards
- Civil Contingencies Act 2004
- NHS Constitution
STATEMENT OF THE CHIEF EXECUTIVE’S RESPONSIBILITIES AS THE ACCOUNTABLE OFFICER OF THE TRUST
The chief executive of NHS England has designated that the chief executive should be the accountable officer of the trust. The relevant responsibilities of accountable officers are set out in the NHS Trust Accountable Officer Memorandum. These include ensuring that:
- There are effective management systems in place to safeguard public funds and assets and assist in the implementation of corporate governance
- Value for money is achieved from the resources available to the trust
- The expenditure and income of the trust has been applied to the purposes intended by parliament and conform to the authorities which govern them
- Effective and sound financial management systems are in place
- Annual statutory accounts are prepared in a format directed by the secretary of state to give a true and fair view of the state of affairs as at the end of the financial year and the income and expenditure, other items of comprehensive income and cash flows for the year.
As far as I am aware, there is no relevant audit information of which the trust’s auditors are unaware, and I have taken all the steps that I ought to have taken to make myself aware of any relevant audit information and to establish that the entity’s auditors are aware of that information.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in my letter of appointment as an accountable officer.
Salman Desai KAM
Chief Executive Officer Date: 18 June 2025
STATEMENT OF DIRECTORS’ RESPONSIBLITIES IN RESPECT OF THE ACCOUNTS
The directors are required under the National Health Service Act 2006 to prepare accounts for each financial year. The secretary of state, with the approval of HM Treasury, directs that these accounts give a true and fair view of the state of affairs of the trust and of the income and expenditure, other items of comprehensive income and cash flows for the year. In preparing those accounts, the directors are required to:
- Apply on a consistent basis accounting policies laid down by the secretary of state with the approval of the Treasury
- Make judgements and estimates which are reasonable and prudent
- State whether applicable accounting standards have been followed, subject to any material departures disclosed and explained in the accounts
- Prepare the financial statements on a going concern basis and disclose any material uncertainties over going concern.
The directors are responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the trust and to enable them to ensure that the accounts comply with requirements outlined in the above mentioned direction of the secretary of state. They are also responsible for safeguarding the assets of the trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
The directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the accounts.
The directors confirm that the annual report and accounts, taken as a whole, is fair, balanced, and understandable and provides the information necessary for patients, regulators, and stakeholders to assess the NHS trust’s performance, business model and strategy.
By order of the North West Ambulance Service NHS Trust Board
Date…18 June 2025……………… Chief Executive:
Date:… 18 June 2025…………… Director of Finance:
Annual Governance Statement
Scope of responsibility
As Accountable Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the NHS trust’s policies, aims and objectives, whilst safeguarding the public funds and departmental assets for which I am personally responsible, in accordance with the responsibilities assigned to me. I am also responsible for ensuring that the NHS trust is administered prudently and economically and that resources are applied efficiently and effectively. I also acknowledge my responsibilities as set out in the NHS Trust Accountable Officer Memorandum.
The purpose of the system of internal control
The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an ongoing process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of North West Ambulance Service NHS Trust, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control has been in place in North West Ambulance Service NHS Trust for the year ended 31 March 2025 and up to the date of approval of the annual report and accounts.
Capacity to handle risk
Leadership
The Board of Directors has overall responsibility for providing strategic leadership of risk management throughout the organisation, which includes maintaining oversight of strategic risks to achieving the trust’s objectives via the Board Assurance Framework (BAF) and leading by example in creating a culture of risk awareness. The Director of Corporate Affairs is accountable to the Board of Directors and the Chief Executive for North West Ambulance Service NHS Trust’s governance and risk management. The Director of Corporate Affairs, with support from the Head of Integrated Governance, Risk and Assurance, provides clear focus for the management of organisational risks and for coordinating and integrating al of the trust’s risk management arrangements.
The Board of Directors is presented with a quarterly risk management assurance report, containing the BAF and the Corporate Risk Register (CRR), both of which are subject to scrutiny at the Trust Management Committee (TMC) meetings.
Executive Directors of the trust are responsible for the consistent application of the Risk Management Policy within their areas of accountability, which includes maintaining an awareness of the overall level of risk within the organisation, the management of specific risks that have been identified and promoting a risk aware culture within their Directorates. Senior Management Teams scrutinise Directorate, Departmental/Team risk registers at their meetings.
Managers within the trust are responsible for making active use of risk registers to support safe management of their service, management of specific risks that have been identified, promoting a risk aware culture, and ensuring that risk assessments are carried out within their service.
Risk Management Training
Risk management training is incorporated into the trust’s induction programme and annual mandatory training programme.
Each year Board Development sessions on risk management, risk appetite, and the development of the BAF are held with the Board of Directors and these focused sessions provide the Board of Directors with an additional opportunity to discuss and debate the strategic risks and Risk Appetite Statement (RAS) and to understand and define the risk tolerance levels for the organisation, prior to formal approval.
The risk and control framework
Risk Management Policy
The Risk Management Policy was reviewed during 2023/24 and defines the approach taken by North West Ambulance Service NHS Trust in applying risk management awareness to its decision-making processes at all levels. The main objective of this policy is to establish the foundations for a culture of effective risk management throughout the organisation by setting out clear definitions, responsibilities, and processes to enable the principles and practices of risk management to be applied consistently throughout the organisation.
The trust risk scoring matrix has been refreshed to ensure standardisation of risk assessments across the trust. All risks are recorded and managed via the trust-wide risk management system.
Risk management is everybody’s responsibility, and the principles of effective risk management should form an integral component of decision-making at all levels.
Where a risk is identified but cannot be managed without some significant change to the way the organisation operates, it is escalated through the relevant line management structure. The policy also requires risk mitigating action plans to be determined and implemented for those risks that are inadequately controlled.
Board Assurance Framework (BAF)
The BAF is an effective method for the oversight of the organisation’s strategic risks i.e., those which could prevent the trust from achieving its corporate objectives, and links with the trust’s strategic aims, objectives, and vision. It provides structures for evidence to support the Annual Governance Statement (AGS) and as a result, streamlines reporting to the Board of Directors. The BAF has continued to mature into a comprehensive system and is embedded within the organisation’s Integrated Governance Structure.
The BAF includes the following key elements:
- Strategic risks of the trust, aligned to the Executive Director Lead and mapped to a Board Assurance Committee for monitoring;
- A description of the strategic risk, including opening, quarterly, in-year and aspirational target scores;
- Projected forecast for the upcoming quarter, including supporting rationale;
- The corporate risks which link to the strategic risk, including risk scoring;
- Risk appetite category and risk tolerance score;
- Key controls in place to mitigate the risks;
- Assurance regarding the effectiveness of the key controls;
- Any gaps in controls and assurances;
- Action plans to address gaps in controls and assurances.
The BAF is approved by the Board of Directors at the commencement of the financial year and is managed through delegation to its Board Assurance Committees. The Trust Management Committee (TMC) continues to promote effective risk management and leadership whilst overseeing and monitoring the management of the BAF.
The Board of Directors reviews the BAF on a quarterly basis and approves the quarterly position. The final version of the 2024/25 Board Assurance Framework was approved at the end of April 2025, by the Board of Directors.
Risk Management
All departments within Directorates maintain a live, dynamic, and well populated risk register via the Trust system. Risk is a key agenda item on all meeting agendas across the trust. The trust supports its people throughout the organisation to manage risk at the most appropriate level, ensuring there is a clear process for risk escalation. Risks are escalated via Departmental and Directorate risk registers to the Corporate Risk Register in accordance with the Risk Management Policy.
All business cases must include a full risk assessment and Equality Impact Assessment (EIA) prior to formal approval. All efficiency schemes have processes in place to identify and mitigate risks to quality and safety.
Risk Appetite
As part of the cyclical Board Development Programme, the Board of Directors received a focused session pertaining to risk appetite. Collectively, the Board of Directors has assessed its risk appetite, and this is reviewed and approved annually. It is also considered when making decisions.
Risk Management Internal Audit
During 2024/25, our internal auditors conducted an audit to provide assurance that core risk management controls have been adequately designed. The audit opinion was concluded as ‘high assurance’, meaning there is a strong system of internal control which has been effectively designed to meet the system objectives, and that controls are consistently applied in all areas reviewed.
Key findings included:
- There was a robust level of control within the risk management system;
- Areas of good practice included the Risk Management Policy being ratified by the Audit Committee, with risk escalation and de-escalation processes in place across the trust;
- Roles and responsibilities of all staff including the Chief Executive, Director of Corporate Affairs, executives and senior management teams are clearly defined;
- Roles and responsibilities of the trust’s governance structure including the Board of Directors and Audit Committee are clearly defined;
- Risk management training requirements are clearly defined, with monitoring of compliance undertaken by the risk management team;
- Clear processes are in place for the identification, assessment and scoring of risks;
- Audit Committee is assigned oversight of risk management processes, in line with the HFMA defined best practice;
- Assurance routes were clearly defined and the trust receives comprehensive risk management reports detailing material risks, control measures, and ongoing actions.
Quality Governance
Quality governance is overseen via the trust’s Quality and Performance Committee which monitors the delivery of the Trust’s Quality Strategy and compliance with the Care Quality Commission (CQC) regulatory requirements under the Health and Social Care Act (2008, 2015) and the Health and Care Act 2022.
The work of the Quality and Performance Committee is supported by the Trust Management Committee (TMC). The Trust Management Committee (TMC) is supported by the Clinical and Quality Group, Health, Safety, Security, & Fire Group, Emergency Preparedness Resilience & Response (EPRR) Group, and the Diversity and Inclusion Group.
In line with the Patient Safety Incident Response Framework (PSIRF) the trust has a Complex Case Review Group (CCRG) and Patient Safety Event Cases (PSEC) meeting. The purpose of these arrangements is set out in the Patient Safety Incident Response Policy and Plan which describes how weekly decision-making governance meetings operate with delegated powers, to review patient safety events from escalation within service lines and make decisions on the appropriate level of response. The Patient Safety Event Cases (PSEC) meeting has delegated responsibility for the consideration of events for Patient Safety Incident Investigation (PSII) or a patient safety learning response for oversight of outcomes. The Quality and Performance Committee maintains oversight of these processes, to provide assurance to the Board of Directors that we are meeting national response standards.
The Quality and Performance Committee receives assurance from an Integrated Performance Report (IPR) which provides oversight against the relevant sections of the NHSE Oversight Framework (2021) including quality indicators, patient experience, patient outcomes, performance, and effectiveness. It also reports on the actions required by national patient safety alerts, progress and accountability.
The Quality and Performance Committee workplan is set to ensure the Committee receives assurances that the trust is safe, effective, caring and responsive to people’s needs and well led. The Committee request and receive additional assurances throughout the annual cycle via a series of deep dives which are focused on areas where the Board of Directors requires additional information or assurances.
Clinical Risk Management
Clinical risk is monitored via the trust’s Clinical and Quality Governance Group and Quality and Performance Committee.
Whilst clinical risk management is everyone’s responsibility, it is managed on a day-to-day basis by operational and clinical staff and is collaboratively monitored by the Corporate Affairs Directorate, Quality Directorate and the Medical Directorate. Clinical risk is reported through the integrated governance, risk and compliance system, Datix Cloud IQ (DCIQ), which allows themes and trends to be identified to inform wider organisational learning.
All clinical practices are carried out using the best available clinical evidence base; this includes advice that is given to patients via telephone as well as advice and clinical interventions performed when our clinicians are in face-to-face situations. In the former, the evidence base is largely taken from the papers published in the UK. For the latter, the evidence base is the Joint Royal Colleges Ambulance Liaison Committee’s (JRCALC) latest clinical guidelines.
The Audit Committee reviews the establishment and maintenance of an effective system of governance, risk management and internal control, across the entire organisation’s activities. This includes activities that are both clinical and non-clinical.
Corporate Governance
There are clear Terms of Reference (ToR) for each Board Assurance Committee and executive-led groups.
There were three Board Assurance Committees, chaired by a Non-Executive Director (NED) that oversaw risk management, both clinical and non-clinical and these were:
- Audit Committee, which sought assurance over the risk management processes and control in place rather than the content and management of individual risks themselves.
- Quality and Performance Committee.
- Resources Committee.
The trust completed a full review of the governance structure during Q4 of 2023-24 and the new governance framework which was established from 1st April 2024 has the following aims:
- Streamline processes, and clarifies governance member roles
- Simplify, clear governance structure with improved executive assurance
- Improve decision-making agility
- Reduce the number of Committees
- Improve accountability
- Reduce the administrative burden.
Each year, the trust undertakes effectiveness reviews of all Board Assurance Committees and Groups. During 2024/25, an interim effectiveness review of the newly established executive led groups was completed and the findings and recommendations were reported to the Trust Management Committee (TMC). Progress against any improvement recommendations have been reviewed during the full year effectiveness review meetings.
Full year effectiveness review meetings are an annual assessment of the trust’s governance meetings. A self-assessment was made available to all governance members and based on five key themes:
- Focus
- Engagement
- Team working
- Meeting Effectiveness
- Leadership.
Outcomes of the annual effectiveness reviews have been presented to the governance meetings, along with draft work plans, revised Terms of Reference for discussions and recommendation for approval.
Board Assurance Committees have continued to undertake frequent ‘deep dives’ into key areas of risk during the year. This has been driven by the gaps in assurances highlighted on the Board Assurance Framework (BAF), in a continued drive for strengthening of assurance.
2024/25 Strategic Risks
The key risks for the trust as it moved into 2024/25 focused on patient safety, financial sustainability and value for money, operational performance and workforce recruitment, retention, and culture, regulatory compliance, engagement with system partners and cyber security.
The following list identifies the strategic risks for 2024/25:
- There is a risk that the trust does not provide high quality, inclusive care leading to avoidable harm, poorer patient outcomes and reduction in patient satisfaction.
- There is a risk that the trust cannot achieve financial sustainability impacting on its ability to deliver high quality (safe and effective) services.
- There is a risk that the trust does not deliver improved national and local operational performance standards resulting in delayed care and/or harm.
- There is a risk that the trust will be unable to maintain safe staffing levels through effective attraction, retention and attendance of sufficient suitably qualified staff impacting adversely on delivery of performance standards and patient outcomes.
- There is a risk that the trust does not improve its culture and staff engagement, and this impacts adversely on retention and staff experience.
- There is a risk that non-compliance with legislative and regulatory standards could result in harm and/or regulatory enforcement action.
- There is a risk that the trust does not work together with our partners in the health and social care system to shape a better future leading to poor effects on our communities and the environment.
- There is a risk the trust suffers a major cyber incident due to persistent attempts and/or human error resulting in a partial or total loss of service and associated patient harm.
- There is a risk that the trust attracts negative media attention arising from long delays and harm leading to significant loss of public confidence.
- There is a risk that the that level of uncertainty and unpredictability both nationally and regionally impacts on, or results in, delayed achievement of our strategic priorities and objectives.
Future 2025/26 Strategic Risks
The key risks for the trust as it moves into the new financial year remain focused around quality and patient safety, financial sustainability, operational performance, workforce recruitment, retention and culture, and cyber security.
The following list denotes the key strategic risks identified for 2025/26:
- There is a risk that if the Trust does not provide the right care, at the right time, in the right place, this may lead to avoidable harm and/or poorer outcomes and experience for patients
- There is a risk that if the Trust does not achieve financial sustainability, its ability to deliver high quality (safe and effective) services will be affected
- There is a risk that if the Trust does not deliver against NHS net zero targets, it will impact on the Trust’s ability to contribute towards environmental improvements and delivery of its Green Plan
- There is a risk that if the Trust does not deliver improved sustained national and local operational performance standards across all services, patients may experience delayed care and/or suffer harm
- There is a risk that if the Trust does not create an inclusive environment and look after its people’s wellbeing, safety and development, then it will be unable to attract, retain and maximise the potential of its workforce for the benefit of patients.
- There is a risk that a breach of legislative or regulatory standards could result in avoidable harm and/or regulatory action
- There is a risk that due to the geographical size of the Trust it will be unable to effectively engage with its numerous system partners which may impact on its ability to achieve the medium-long-term plan
- There is a risk that if the Trust suffers a cyber incident, it could result in an inability to deliver a service and associated harm.
- There is a risk that the recent planned changes around the Board over the next 12 months could destabilise the organisation and impact delivery of strategic plans.
- There is a risk that due to the timing of contracting decisions for NWAS commissioned services (PTS and 111), this will impact the development of our strategic priorities and objectives.
- There is a risk that the current financial landscape of the NHS may impact the achievement of the trust’s strategic priorities and performance by reducing the availability of resources both financial and physical.
The Governance Framework
The trust has reviewed its corporate governance arrangements against the NHS Code, a declaration of compliance against all relevant (non-FT) provisions during 2024/25 was reported to Audit Committee and the Board of Directors during April 2025. The trust has declared compliance with all relevant clauses in the Provider Licence.
The Board of Directors recognises its accountabilities and provides strategic leadership with a framework of prudent and effective controls which enables risks to be assessed and managed throughout the organisation.
The Board of Directors sets the strategic direction for the organisation and ensures that resources are in place to meet its objectives. It receives reports at each meeting held in public on the principal strategic risks through a combination of risk management assurance reports, and/or an Escalation and Assurance Reports from the Board Assurance Committees.
The Board of Directors currently meets at least six times per annum and during the reporting period consisted of:
- The Chair plus 5 other Non-Executive Directors, including a Senior Independent Director (SID)
- The Chief Executive Officer and 4 other voting Executive Directors
- 3 non-voting Executive Directors.
During 2024/25, there were changes to the composition of the Board of Directors:
- A new Director of Operations was appointed and commenced in role on 01 July 2024.
- The Chief Executive Officer left the trust on 30 November 2024, and the Deputy Chief Executive/ Director of Strategy, Partnerships, and Transformation was appointed as Acting Chief Executive Officer to provide interim cover until a substantive Chief Executive Officer was appointed. The Acting Chief Executive Officer was successfully appointed as the Chief Executive Officer and commenced in post on 01 January 2025.
- The Director of Quality, Innovation and Improvement left the trust on 31 March 2025. An interim Director of Quality was appointed in March 2025 to provide interim cover until a substantive Director of Quality is appointed.
- Following the announcement of the Chief Executive’s resignation, the Chair’s final term of office (originally due to end 31/1/25) was extended with the approval of NHS England and the support Lancashire and South Cumbria Integrated Care Board (ICB), until 31 July 2025.
The Board of Directors has three key roles:
- Formulating strategy for the organisation.
- Ensuring accountability by; holing the organisation to account for the delivery of the strategy; by being accountable for ensuring the organisation operated effectively and with openness, transparency and candour and by seeking assurances that systems of control are robust and reliable.
- Shaping a healthy culture for the Board of Directors and the organisation.
Quality is a central element of all Board of Directors meetings. The Integrated Performance Report (IPR), which continues to be developed and enhanced, is aligned with the System Oversight Framework (SOF) with focus on key quality indicators.
A patient or a staff story opens each meeting of the Board, to ensure that the focus on quality of patient care and the safety and wellbeing of our people remains at the core of all Board of Directors’ activity and decision-making.
At each Board of Directors meeting, the Board reviews reportable events which includes Patient Safety Incident Investigations (PSIIs), serious case reviews, reportable events to the Health and Safety Executive (HSE), claims, and coroner’s inquests. The Clinical and Quality Group, Health, Safety, Security & Fire Group, and the Quality and Performance Committee review these matters in greater detail along with complaints and concerns, and learning for clinical and non-clinical incidents is disseminated via the trust’s local Learning Forums, held within geographical areas and for clinical and patient safety learning and improvement at the Regional Clinical and Improvement Group.
During the year, there has not been any nationally defined ‘Never Events’ as a result of the care and services provided by the trust.
The Trust Management Committee (TMC) meets monthly and is accountable for oversight of the operational management of the trust. The Trust Management Committee (TMC) provides the Board of Directors with assurance concerning all aspects of delivering the trust’s operations and strategic direction and associated operational plans. The remit also extends to management of organisational risk and governance; investment and disinvestment; performance delivery; horizon scanning; strategy and policy development, interpretation and implementation, and stakeholder and partner engagement.
Arrangements are in place through the Board of Directors and Board Assurance Committees meetings throughout 2024/25 are detailed on page116 of the Annual Report.
There is a statutory requirement for all NHS trusts to hold a Provider Licence issued by NHS England. Whilst there is no obligation for NHS provider trusts to produce a formal document detailing compliance with the Licence, there is an expectation for regulators, that should they seek assurance, the trust will be able to declare compliance and evidence the basis on which that declaration is made. The trust self-certified as being compliant with the conditions of the Provider Licence for 2024/25 and reported this through Audit Committee mid 2024/25. Full year compliance for 2024/25 will be reported through Audit Committee at the start of 2025/26.
During Q1 2025/26, the trust will be commissioning an externally facilitated Well-Led review.
Workforce
The trust has an approved 3-year People Strategy with a supporting implementation plan reinforced by a set of clear measures. The Strategy was refreshed in 2024 in order to take account of the changing national context of the Ambulance Culture review. The NWAS People strategy looks forward over a three-year period, with a supporting set of annual objectives focussed on improvements and developments. Progress against implementation of the strategy is monitored on behalf of the Board of Directors through the Resources Committee and the associated workforce governance structures, with key projects also overseen by the Corporate Programme Board (CPB).
The trust’s approach to workforce planning and development takes account of the NHS England priorities and operational planning guidance, issued each year, to take account of national developments, such as the NHS Long Term Workforce Plan. The Trust’s workforce planning process seeks to ensure appropriate and robust governance and monitoring at the strategic, tactical and operational levels. These plans are reviewed regularly with assurance on the progress of plans provided to the Board of Directors, Resources Committee and the Trust Management Committee (TMC).
At a strategic level, the operating plan for the year takes account of the projected turnover, required recruitment, along with any growth and planned transformational changes. Forecasts are made to consider the potential usage of Bank and Agency staffing. Sickness absence is also considered to take account of trends and strategic targets to reduce sickness absence. Plans are signed off at a Board level and submitted regionally ahead of a national review.
At a tactical level, agreed plans are actively monitored with service lines and Finance on a monthly basis to identify and address any developing trends. The planning process is dynamic which allows the opportunity to discuss emerging issues that may impact on the plans and allow flexibility to accommodate changes. The People Directorate work closely with the Director of Finance to ensure that both the workforce and finance plans triangulate on a monthly basis.
The trust produces workforce information in the form of workforce dashboards and workforce plans for the frontline workforce within Paramedic Emergency Service (PES), Patient Transport Service (PTS) as well as Integrated Contact Centres (ICC). The Board of Directors and Senior Management Teams receive monthly reports on workforce data through the Integrated Performance Report (IPR) and supporting workforce dashboards, which demonstrates the position against planned establishment.
Operationally, the People Directorate work closely with service lines with regular meetings to discuss the current workforce position against the planned position in accordance with the operating plan. Discussions include the emerging recruitment requirements and the position of fill rates for planned courses. Managers work within the context of the financial boundaries and governance processes, especially regarding the appropriate use of agency within the delegated ceiling and agency framework. The People and Finance teams work closely to ensure clear triangulation between the workforce and financial position.
The anticipated turnover rate is mapped throughout these plans to allow a forward view over the next twelve months allowing service lines to visualise the anticipated workforce position. For Paramedic staffing, these detailed annual plans sit within the context of a five-year plan focused on ensuring appropriate Paramedic supply which is reviewed through regular engagement with NHS England and Higher Education Institute (HEI) partners.
Throughout 2024/25, assurance has been provided against the workforce and recruitment plans to the People and Culture Group and onward assurance is provided to the Trust Management Committee (TMC). Ad hoc reports have also been provided on specific risks associated with the workforce plan to Board Assurance Committees and safe staffing has been separately identified as a BAF risk in 2024/25.
To ensure the trust is able to deliver its efficiency programme, a Vacancy Control Panel (VCP) meets on a weekly basis to assess recruitment requests to ensure that this is considered against local efficiency plans and waste reduction targets. Requests are scrutinised and considered prior to recruitment commencing. It should be noted that recruitment to frontline posts is considered and agreed as part of the Operating Plan submission.
The trust utilises the Model Ambulance dashboard and Corporate Benchmarking metrics to gain an overview of clinical and non-clinical workforce composition including staff numbers, pay costs, skill mix ratios and productivity in terms of clinical outputs. This in turn supports the Trust to identify potential opportunities to improve efficiencies and productivity.
The trust has successfully continued to reduce agency usage through improved workforce planning with a focus on prioritising alternative options above using agency staff. A small amount of agency is factored into our operating plan to support ad hoc clinical vacancies within the Integrated Contact Centres (ICC’s).
The trust’s paramedic workforce supply continues to be strengthened through longer term strategic plans to develop and support internal development routes to paramedic through degree apprenticeships, to increase external supply, to develop partnerships and to actively recruit.
The trust is fully compliant with the registration requirements of the Care Quality Commission.
The trust has published on its website an up-to-date register of interests, including gifts and hospitality, for decision-making staff (as defined by the trust with reference to the guidance) within the past twelve months, as required by the ‘Managing Conflicts of Interest in the NHS’ guidance.
As an employer with staff entitled to membership of the NHS Pension Scheme, control measures are in place to ensure all employer obligations contained within the Scheme regulations are complied with. This includes ensuring that deductions from salary, employer’s contributions and payments into the Scheme are in accordance with the Scheme rules, and that member Pension Scheme records are accurately updated in accordance with the timescales detailed in the Regulations.
Control measures are in place to ensure that all the organisation’s obligations under equality, diversity and human rights legislation are complied with.
The trust has undertaken risk assessments on the effects of climate change and severe weather and has developed a Green Plan following the guidance of the Greener NHS programme. The trust ensures that its obligations under the Climate Change Act and the Adaptation Reporting requirements are complied with.
Review of economy, efficiency and effectiveness of the use of resources
The trust secures the economic, efficient, and effective use of resources through a variety of methods, including:
- A well-established policy framework including Standing Orders, Standing Financial Instructions and Scheme of Delegation.
- An organisational structure which ensures accountability and challenge through the Integrated Governance Structure.
- Effective Corporate Directorates responsible for revenue and capital planning and the control and management of resources.
- A clear planning process, aligned with our Integrated Care System, resulting in the approval of an annual financial plan by the Board of Directors.
- Budgets delegated across the trust, with budget holders receiving detailed monthly financial reports.
- Senior Management Teams and Budget holders continue to play an active part in ongoing review of financial performance and delivery of efficiency programmes.
- Detailed financial reporting to the Trust Management Committee (TMC) and the Resources Committee including income and expenditure; statement of financial position; progress on the achievement of efficiency and productivity programmes; capital expenditure programmes; and key financial risks.
- The Trust Management Committee (TMC) takes a lead in financial planning, delivery and taking actions for recovery to bring variances back to plan when required.
- The Trust Management Committee (TMC) throughout the year regularly reviews performance against clinical, performance, workforce, and financial indicators.
- The Trust continues to invest time and resources to improving systems and controls to deliver a more embedded range of monitoring and control processes.
- The Vacancy Control Panel (VCP), ensures there is an established vacancy prior to recruitment alongside the review of financial performance for that service line, including achievement of efficiency targets, before approval to recruit.
The in-year use of resources is closely monitored by the Board of Directors and the following Board Assurance Committees:
- Audit Committee
- Resources Committee
- Quality and Performance Committee.
The Audit Committee scrutinises and challenges the effectiveness of the trust’s financial and governance arrangements to manage finance and secure value for money (VFM). The trust employs several approaches to ensure the best value for money in delivering its services. Benchmarking is used to provide assurance and to inform and guide service redesign. This leads to improvements in the quality of services and patient experience as well as financial performance.
The governance arrangements are supported and strengthened by an effective internal audit plan. The external auditors provide a key independent source of information for the Audit Committee membership, and the public, in determining and reporting on the financial statements and value for money arrangements across the trust. Through this process, the trust has gained independent and objective assurance to the Audit Committee and the Board of Directors that the trust’s risk management, governance and internal control processes are operating effectively.
The trust has a dedicated, qualified Anti-Fraud Specialist (AFS) supported as required by other AFS. Any concerns can be directed to the team and, any information is treated in the strictest confidence.
External Auditors, Internal Auditors, and Anti-Fraud report to each meeting of the Audit Committee and meet the membership of the Audit Committee without any management present.
Information governance
The trust uses the Datix Cloud IQ (DCIQ) system to capture data breaches via the incidents module. During 2024/25 financial year (April 2024 to March 2025), 157 data breaches were reported. Each information breach is risk scored against the trust risk matrix and investigated. The main category of reported data breaches was ‘data confidentiality’. Five incidents were deemed a high risk to the rights and freedoms of individuals and were reported externally via the Data Security Protection Toolkit (DSPT) to the Information Commissioners office (ICO).
- One breach involved unlawful disclosure of a member of staff’s personal details, including home address, resulting in threats to the data subject. The ICO issued advice, and no further action was requested.
- One breach related flu vaccination status of circa 200 staff being shared inappropriately internally. This also resulted in advice from the ICO, and no further action was requested.
- The following three breaches are pending an outcome from the ICO:
- Concern raised due to internal sharing of confidential information.
- Inappropriate disclosure of address details as part of a disciplinary procedure.
- Internal trust system pre-dating the General Data Protection Regulations (GDPR), therefore no Data Protection Impact Assessment (DPIA) was mandated at the time, allowing external sharing of staff data.
Learning from information incidents and breaches are discussed at the Information and Cyber Governance Group and action plans developed accordingly for management of local issues and sharing learning.
Data quality and governance
The Data Quality Team has worked against a programme of data quality audits throughout 2024/25 to support key priorities of the trust. This has included auditing incident reporting, within the DCIQ system. This is currently supporting an ongoing project looking at the accuracy and reporting of unavailability time recorded for ambulance crews. Monitoring the reporting of our trust Electronic Patient Record (EPR) has been enhanced to include public health related fields to identify when they may not have been accurately recorded. The Data Quality Team have produced reporting and developed ways of working with our operational teams to investigate and rectify erroneous time stamps relating to negative time travel and high times, both of which have assisted in the mandatory submissions of the Ambulance Data Set and patient level costings respectively.
The prioritisation of the Data Quality programme of work will continue to follow and complement ongoing reporting priorities within the Data Insights and Intelligence roadmap. This will allow for monitoring reports to organically grow for Information Asset Owners (IAO) and Information Asset Administrators (IAA) to undertake their responsibility to proactively view and improve processes to ensure the quality of data being produced within their systems.
Review of effectiveness
As Accountable Officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review of the effectiveness of the system of internal control is informed by the work of the internal auditors, clinical audit and the executive managers and clinical leads within the NHS trust who have responsibility for the development and maintenance of the internal control framework. I have drawn on the information provided in this annual report and other performance information available to me. My review is also informed by comments made by the external auditors in their management letter and other reports. I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the board, the audit committee, quality and performance committee, the resources committee and a plan to address weaknesses and ensure continuous improvement of the system is in place.
My review is informed in several ways:
- The Audit Committee’s Annual Report for 2024/25.
- The Head of Internal Audit provides me with an independent opinion of the overall arrangements for gaining assurance through the Board Assurance Framework (BAF), and the controls reviewed as part of the internal audit work.
- Executive Directors and senior managers within the organisation who have responsibility for the development and maintenance of the system of internal control provide me with assurance.
- The Board Assurance Framework (BAF) itself provides me with evidence of the effectiveness of controls that manage the key risks to the organisation achieving its strategic aims and objectives have been reviewed.
- The overall rating of ‘Good’ and ‘Outstanding’ for the trust’s urgent and emergency care responsiveness domain, by the Care Quality Commission (CQC) during their last inspection of the trust.
My review is also informed by:
- The NHS Data Security and Protection Toolkit.
- Assessment against the NHS Counter Fraud Authority Standards for Providers.
- Peer reviews within the ambulance service sector.
- Internal audit reports.
- Clinical audit findings.
- External audit findings.
- External consultancy reports on key aspects of the trust’s governance.
The Board of Directors seeks assurance that risk management systems and processes are identifying and managing risks to the organisation appropriately through the following:
- At least annually, a review of the effectiveness of the trust’s system of internal control.
- The Board of Directors ensures that the review covers all material controls, including financial, clinical, operational, and compliance controls, and risk management systems.
- A review of the Risk Management Policy.
- A quarterly presentation of the Board Assurance Framework (BAF) at Board of Director meetings.
- Monthly integrated performance reporting at Board of Directors meetings, outlining achievements against key performance, safety and quality, and finance indicators.
- Assurance reports at each meeting, providing information on progress against compliance with national standards.
- Assurance from internal and external audit reports that the trust’s risk management systems are being implemented.
The follow-up of internal audit recommendations is regularly monitored at the Trust Management Committee (TMC), Internal Audit, and Audit Committee. The trust has a comprehensive risk-based internal audit plan in place and this programme was delivered during 2024/25. The outcome of the 2024/25 internal audit programme, reported via the Head of Internal Audit Opinion, which overall gave the trust Substantial Assurance – that there is a good system of internal control designed to meet the organisation’s objectives, and that controls are generally being applied consistently.
During the year, the following audit assurance outcomes were reported:
- 3 audits were assessed as High Assurance
- 8 audits were assessed as Substantial Assurance
- 2 audits were assessed as Moderate Assurance
- 0 audits were assessed as Limited Assurance
- 0 audits were assessed as No Assurance.
The trust’s internal auditors have also supported the organisation in strengthening arrangements in respect of risk management and internal control. The 2024/25 Internal Audit Programme, audit work has provided assurance across the trust’s critical business systems, namely, financial systems, information and technology, performance, quality and safety, workforce, governance and risk, and legality. Recommendations made have resulted in actions taken to further strengthen systems and controls in year.
The trust’s internal auditors, as required by NHS England to assess and provide assurance based upon the validity of the trust’s intended Data Security Protection Toolkit (DSPT) submission. The self-assessment against the toolkit deviated only minimally from the Independent Assessment, and as such, gave the trust Substantial Assurance. Across the National Data Guardian Standards, assurance ratings are based on a mean risk rating score at the National Data Guardian (NDG) standard level. As a result of this, this gave the overall assurance level across the 10 National Data Guardian Standards as Substantial Assurance.
During 2024/25, the trust’s Clinical Audit department participated as a provider of information to the national clinical audits, and these are as follows:
- National Ambulance Clinical Quality Indicators, a national audit of the care of the patient who were assessed by ambulance clinicians are:
- Suffering a pre-hospital cardiac arrest;
- Suffering a pre-hospital heart attack;
- Suffering from falls in older adults;
- Recontacts within 24 hours.
Conclusion
Following my review and taking into account the contents of this report and the evidence-based assurance seen at the Board Assurance Committees, I can confirm that no significant internal control issues have been identified.
Signed:
Salman Desai
Chief Executive Date: 18 June 2025
Remuneration Report
Nominations and Remuneration Committee
The board of directors has established a Nominations and Remuneration Committee that advises them with regard to the appropriate remuneration and terms of service of the chief executive and other executive directors including:
- At least annually review the structure, size and composition (including the skills, knowledge and experience) of the board of directors
- Identify and appoint candidates to fill the position of chief executive and any director vacancies in conjunction with NHSE
- With regard to the chief executive, directors; trust secretary and other very senior managers; in conjunction with NHSE where required and ensuring that officers are fairly rewarded for their individual contribution to the trust – having proper regard to the trust’s circumstances and performance and to the provisions of any national arrangements for such staff
- Arrangements for termination of employment and other contractual terms.
The members of the committee are the chair and non-executive directors. The chief executive, other directors and any other officers in attendance are not present for discussions about their own remuneration and terms of service.
Policy on Remuneration
The determination of salaries for senior managers for 24/25 onwards is informed by national guidelines regarding very senior managers’ (VSM) pay which cover the chief executive, executive director, and the majority of director posts and where appropriate are approved by NHS England.
Contracts of Employment
The Executive Leadership team are employed on full time contracts which meet the current requirements of the national guidance. The period of notice required for these posts is six months. Termination payments are governed by guidelines set by HM Treasury that allow for compensation to be paid in relation to the notice period given, together with any statutory redundancy settlement, if applicable. Any exceptions to this require the prior approval of NHS England and the Treasury. No such termination payments have been made in 24/25.
Performance Related Pay
The broad arrangements for annual salary uplifts and the performance bonus scheme are specified in The Pay Framework for very senior managers in strategic and special health authorities, primary care trusts, and ambulance trusts (June 2013) and in the subsequent guidance on pay for very senior managers in NHS trusts and foundation trusts (February 2017).
For 24/25 VSM the annual pay uplift was recommended under the remit of the Senior Salaries Review Body (SSRB). The government agreed to accept the recommendation of the SSRB:
- The application of the 5% VSM pay award recommended by the Senior Salaries Review Body and NHS England, to all directors employed on VSM contracts at 1 April 2024.
No provisions were made within the pay award for the application of bonuses. The Nominations and Remuneration Committee agreed with the recommendations and details of senior managers’ remuneration and pensions are shown in the following tables.
Salaries and Allowances 24/25 (subject to audit)
Table 1: Single Total Figure Table
Table 2: Pension Benefits (subject to audit)
Note: CETV figures are calculated using the guidance on discount rates for calculating unfunded public service pension contribution rates that was extant at 31 March 2025. Where calculations have resulted in negative impact the amount is shown as zero (in line with guidance).
Notes to accompany remuneration tables:
Auditable Content
Salaries and Allowances 24/25
Pension benefits
Staff numbers and costs
Exit packages
Pay multiples
Pay Multiples (subject to audit)
Entities are required to disclose pay ratio information and detail concerning percentage change in remuneration concerning the highest paid director. The banded remuneration of the highest paid director in North West Ambulance Service NHS Trust in the financial year 2024/25 was £170,000-175,000k (2023/24, £200,000-205,000k).
The range of staff remuneration during 24/25 was £20,000 – £25,000 to £170,000 – £175,000 (2023/24 £20,000 – £25,000 to £200,000- £205,000). The table below shows percentage changes in remuneration within 2024/25:
| Average | Staff Costs Average | Highest Paid Director |
| 2024-25 | 41,771 | 172,500 |
| 2023-24 | 42,134 | 202,500 |
| -0.9% | -14.8% |
It must be noted that the chief executive who is the highest paid directors left NWAS in November 2024.
Reporting bodies are required to disclose the relationship between the remuneration of the highest paid director in their organisation and the 25th percentile, median and 75th percentile of remuneration in organisation’s workforce. Total remuneration is further broken down to show the relationship between the highest paid director’s salary component of their total remuneration against the 25th percentile, median and 75th percentile of salary components of the organisation’s workforce.
Total remuneration includes salary, non-consolidated performance-related pay, benefits-in-kind, but not severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pensions. The relationship to the remuneration of the organisation’s workforce is disclosed in the below table.
| 25th Percentile Pay Ratio | Median Pay Ratio | 75th Percentile Pay Ratio | |
| 2024-25 | 5.6:1 | 4.6:1 | 3.3:1 |
| 2023-24 | 6.7:1 | 5.3:1 | 3.8:1 |
In 2023/24 employees were paid a bonus that was agreed in 2022/23 and in addition a pay award of 5% was paid as well. This leads to slight change in ratios in the table above.
Table below shows the difference between salary and full remuneration and the relation to the highest paid director.
| 2024/25 | 25th Percentile | Median | 75th Percentile |
| Staff component of pay (£) | 30,509 | 37,338 | 52,573 |
| Total pay and benefits excluding pension benefits (£) | 30,597 | 37,407 | 52,655 |
| Pay and benefits excluding pension: pay ratio for highest paid director | 5.6:1 | 4.6:1 | 3.3:1 |
Cash Equivalent Transfer Values – A Cash Equivalent Transfer Value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valued are the member’s accrued benefits and any contingent spouse’s pension payable from the scheme. A CETV is a payment made by a pension scheme or arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension figures shown relate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which disclosure applies. The CETV figures and the other pension details include the value of any pension benefits in another scheme or arrangement which the individual has transferred to the NHS pension scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in the scheme at their own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries.
Real Increase in CETV – This reflects the increase in CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation, contributions paid by the employee (including the value of any benefits transferred from another scheme or arrangement) and uses common market valuation factors for the start and end of the period.
Compensation for Early Retirement or Loss of Office
There were no such payments made during 24/25.
Payments to Past Directors
There were no such payments made during 24/25.
Staff Report
Executive Directors
During the year, the trust had eight director positions for which VSM salaries are payable.
In addition, the trust appointed to four further VSM positions as part of the senior operational restructure. These posts operate at a sub-board level.
For further details please see the Remuneration Report table.
Non-Executive Directors
During the year, the trust had the following non-executive directors in place:
- Five non-executive directors on non-executive pay bands
- Chair of the trust board on chair pay band
Whilst non-executive directors and the trust board chair are senior managers of the organisation, they are not trust staff and their terms and conditions are determined by NHSE.
The chair’s terms of office were due to end on 31 January 2025 however, following approval by NHS England, were extended to 30 July 2025 to provide stability to the board during a period of change within the executive team. To support this further, the terms of office for a non-executive director were also extended to 30 November 2025 by NHS England.
For further details please see the Remuneration Report table.
Senior Manager by Band
The trust’s definition of a senior manager is the chief executive and director posts. For a breakdown of salary bands, please refer to the Salaries and Allowances detailed within the Remuneration Report.
Staff Numbers and costs (subject to audit)
The breakdown of staff at 31 March 2025 is as follows:
| Average number of employees (WTE basis) | |||||||
| Permanent Number | Other Number | 2024/25 Total Number | 2023/24 Total Number | ||||
| Medical and dental | 2 | – | 2 | 4 | |||
| Ambulance staff | 6,187 | – | 6,187 | 5,978 | |||
| Administration and estates | 676 | 3 | 679 | 666 | |||
| Healthcare assistants and other support staff | 97 | – | 97 | 120 | |||
| Nursing, midwifery and health visiting staff | 123 | 5 | 128 | 120 | |||
| Nursing, midwifery and health visiting learners | – | – | – | – | |||
| Scientific, therapeutic and technical staff | 5 | – | 5 | 2 | |||
| Healthcare science staff | – | – | – | – | |||
| Social care staff | – | – | – | – | |||
| Other | – | – | – | – | |||
| Total average numbers | 7,090 | 8 | 7,098 | 6,890 | |||
Table: Staff numbers and costs
Staff Composition and Staff Policies
NWAS continues aiming towards having a workforce which is representative of the communities we serve across the North West and being an employer of choice for all.
As required in the NHS contract, we continued to meet all our statutory and regulatory reporting requirements in relation to EDI – including submitting our its Workforce Disability Standard, Workforce Race Equality Standard, Gender Pay Gap and Equality Delivery System data.
Note: the headlines relating to the WDES, WRES and Gender Pay Gap below are based on data which was extracted and 31 March 2024 and submitted in subsequent months. Data for period of 1 April 2024 – 31 March 2025 will be published later in the year.
NHS Equality Delivery System (EDS)
The EDS is an NHS England framework that helps NHS organisations improve the services they provide for their local communities, and create better working environments, free of discrimination, for those who work in the NHS, while meeting the requirements of the Equality Act 2010.
There are three main areas that EDS focuses on, with evidence for each area assessed by a panel of stakeholders:
- Domain 1 – Commissioned or provided services
- Domain 2 – Workforce health and well-being
- Domain 3 – Inclusive leadership
The assessment was undertaken between December 2024 – January 2025, with the findings submitted to NHS England ahead of the 28 February deadline.
This year, our organisational rating was 18, placing the trust at ‘developing’ – sustaining last year’s position. Further efforts around the recording and utilisation of EDI monitoring to drive improvements could help increase the organisational rating in future assessments.
The full evidence pack used for the assessment can be seen on the NWAS website.
Workforce Disability Equality Standard
We continued to see an increase in the numbers of staff declaring that they have a disability or long-term condition. At the end of March 2024, 7.8% of all staff had declared they had a disability – an increase from 6.5% in 2023 and 5.0% in 2022.
Figures around the relative likelihood of disabled staff compared to non-disabled staff entering the formal capability process further deteriorated from the previous year’s score, meaning that that disabled staff were over one –and –a half times more likely to enter the capability process compared to non-disabled staff. Numbers of staff affected were however, in single figures.
Whilst the actual experience of negative behaviours decreased for disabled staff, there was a notable increase in the proportion of disabled staff reporting negative experiences when they occur. On the whole, NHS Staff Survey results since 2018 consistently show that a greater percentage of disabled staff report their experiences of bullying, harassment or abuse compared to non-disabled staff.
Around one in three disabled staff reported feeling satisfied with how the organisation values their work, and this is the highest positive response since reporting on this metric started in 2018. Additionally, the difference between disabled and non-disabled staff has significantly narrowed on this question in comparison to the previous year.
The detailed WDES report was published on the trust website and can be accessed for more details.
Workforce Race Equality Standard
The WRES figures showed a consistent increase in the number of BME staff in the organisation since 2019. There were 100 more BME staff in the organisation on 31 March 2024, compared to the same date in March 2023.
Overall, the experiences of BME staff as seen through the WRES indicators showed improvements. This was particularly apparent through the data extracted from the NHS Staff Survey which saw considerably more responses from BME staff in 2023 compared to 2022.
Figures in Indicators 5 – 7 showed fewer BME staff experiencing bullying, harassment or abuse from the public or colleagues, and more BME staff feeling that organisation acts fairly in terms of career progression. It was also encouraging to see that improvements in figures are helping narrow the gap in experience between BME and white staff.
However, recruitment data showed that white staff are more than one –and –a half times more likely to be appointed compared to BME applicants – which is a worsening of the previous year’s position. This is despite significantly more BME applicants being shortlisted, and an increase in the number of BME staff being appointed.
Indicator 3 relating to the relative likelihood of BME staff entering the formal disciplinary process compared to white staff identified an area of significant concern. The data in this Indicator showed that BME staff are over two –and –a half times more likely to enter the formal disciplinary process compared to their white colleagues.
An exploration of the disciplinary data found that out of less than 100 formal disciplinary cases in 23/24, around 15 related to BME staff and are largely concerned with lower-level incidents. While these numbers were low when compared to the overall BME and white staff total, the BME cases equated to 16% – when the proportion of BME staff in the organisation is only 6%. Work is continuing to improve this position.
The detailed WRES report was published on the trust website and can be accessed for more details.
Gender Pay Gap
Female representation in the NWAS workforce has consistently increased over a number of years. As of 31 March 2024, 53.13% of staff were female (52.14% in 2023, 51.60% in 2022). Additionally, the majority of the workforce (55.43%) in the Operations directorate were female, and women accounted for half of all staff across the corporate directorates.
The percentage of women in the lower and lower middle quartiles fell for the first time, while increasing in the upper middle and upper quartiles. The most sizable increase was in the upper quartile, where female representation stood at 44.06% – an increase of 5% on the previous year.
The hourly mean/average pay gap continued to narrow and was at 7.27%. While still a significant gap, this was however the lowest average figure since we started reporting. This reflected the increasing representation in the higher pay quartiles and the impact of work around progression.
On the other hand, the median hourly gap increased to 11.17%. This is largely because of the higher proportion of female than male staff in the entry pay bands.
The WRES, WDES and GPG data reflects the ongoing work to support all our staff groups and address inequalities in the workplace. While there have been some improvements across a number of key areas, we recognise that there remains a considerable difference in the experiences of BME, disabled and female staff in the organisation.
Figure: Ethic Grouping – All employees at 31 March 2025
Figure: Gender – Senior managers at 31 March 2025
Figure: Gender – Executive and non-executive directors 31 March 2025
Sickness Absence Data
Total days lost in 24/25 due to sickness is 108,772.
Staff Turnover Percentage
The turnover percentage for permanent and fixed term employees up to 31 March 2025 was 8.28%.
Trade Union Facility Time
The trade union (Facility Time Publication Requirements) Regulations 2017 came into force on 1 April 2017. The regulations require public sector employers to publish information on how much time is spent by their union officials on paid ‘trade union facility time’ and is detailed for 24/25 in the tables below:
| Number of employees who were relevant union officials during the relevant period | 103 |
| Full time equivalent employee number | 95.93 |
| Percentage of time spent on facility time | |
| Percentage of time | No. of employees |
| 0% | 16 |
| 1-50% | 76 |
| 51%-99% | 1 |
| 100% | 10 |
Paid trade union activities
Time spent on paid trade union activities as a percentage of total paid facility time hours calculated as: (total hours spent on paid trade union activities by relevant union officials during the relevant period/total paid facility time hours x 100) was 0.0%.
| Percentage of pay bill spent on facility time | |
| First Column | Figures |
| Provide the total cost of facility time | £597,871 |
| Provide the total pay bill | £386,087,000 |
| Provide the % of the total pay bill spent on facility time, calculated as: (total costs of facility time/total pay bill x 100) | 0.2% |
Table: Trade union facility time 24/25
Expenditure on Consultancy
Expenditure on consultancy totalled £146k during 24/25.
Ill Health Retirements
During 24/25 there were seven ill health retirements.
Off-Payroll Engagements
There are no off-payroll engagements to disclose during 24/25.
Exit Packages (Subject to Audit)
There were no exit packages during 24/25.
Independent Auditor’s Report to the Board of Directors of North West Ambulance Service NHS Trust
Annual Accounts 24/25
Appendix – Glossary of Terms
(This glossary does not form a part of the statutory accounts)
Statement of Comprehensive Income
- Income and Expenditure
Often called a Profit and Loss account or an Income and Expenditure account. Public sector accounts tend to use the term Income and Expenditure to indicate that they are non-profit making organisations.
- Income from activities
Income from patient care activities of the trust, usually from Clinical Commissioning Groups as the principle commissioner of services.
- Other operating income
Income from non-patient care services such as commercial training, research funding etc.
- Operating surplus
The surplus generated by the normal operations of the trust before taking into account interest, depreciation, and amortisation
- Depreciation
When a fixed asset is purchased, the cost of that asset needs to be charged to the income and expenditure account over the life of the asset to recognise the contribution of that asset to the work of the trust in each year of ownership. On purchase of a fixed asset, the expected life is assessed, and the cost is spread over that life. The value of the asset therefore diminishes, or depreciates, over time.
- Amortisation
Where depreciation applies to tangible fixed assets, amortisation is the same process for non-tangible fixed assets, such as loans to the trust.
- Profit / (loss) on disposal of fixed assets
The difference between the value of an asset in the balance sheet and the actual sale price of the item. This could be equipment or buildings.
- Public Dividend Capital (PDC)
PDC originated in NHS trusts as the difference between the valuation of its assets and liabilities on establishment as an NHS trust. This originating debt is deemed an asset of the secretary of state and equates to taxpayers’ equity in the organisation. The trust has to make a return on this capital equivalent to 3.5% per annum, and this amount has to be paid over to the Treasury. The original debt can increase over time due to the allocation of additional capital funds and is repayable over time.
Statement of financial position
- Fixed Asset / Non-Current Assets
An asset that has a life that extends beyond the current financial year and that will generate economic benefits in future accounting periods – as opposed to current assets, which are realisable immediately or in the next accounting period. Fixed assets are typically equipment or buildings.
- Current Assets
These are assets that are held on the balance sheet of the organisation that have an immediate cash value. These include stocks, that could be sold and realise cash quickly, debtors that can be collected quickly to realise cash or cash held in a bank account.
- Stock / Inventories
Material held as stock which could be sold to realise cash quickly. Can either be valued at cost where stock is valued in the books at the purchase price or, net realisable value where stock is valued in the books at a value that it could reasonably be expected to fetch if it was sold on the open market today.
- Debtors / Receivables
Money owed to the trust for services provided.
- Creditors / Payables
Money owed by the trust for goods and services received.
- Total Taxpayers’ Equity
See Public Dividend Capital
Notes to the accounts
- Historical Cost Convention
The value of an asset carried in the balance sheet is the amount paid for it on the purchase date.
- Accruals Convention
The accounts are prepared taking account of all income received and receivable, and all expenditure paid and payable for the goods and services delivered and received in the period and are not based on cash receipts and payments in the period.
- Off Balance Sheet
Refers to fixed assets that are in use by the trust, but which are not technically ‘owned’ by the organisation, and therefore do not appear in the balance sheet. An example of this would be operating leases, where equipment, such as vehicles, is leased by the organisation but never comes into our ownership.
- Liquid Resources
Resources that can be released quickly to enable the organisation to settle debts. Typically, cash in hand or in the bank in short term accounts.
- Prepayment
Where the trust has paid in advance for goods or services – for example, quarterly payment in advance for telephone rentals.
- Deferred Income
Income received in the financial year but deferred to a subsequent accounting period because the relevant services will be provided in that future accounting period.
- Reserves
Funds set aside in recognition of a future event, project, or change, where the need has been recognised but the event has not happened.
TERMINOLOGY
- Going Concern Basis
The accounts are prepared on the basis that the trust will still be in existence in the next financial year, and that it will therefore be in a position to recover any debtors due to it, and that it will be around to cover its long term liabilities. If it is likely that an organisation will not be in existence beyond this set of accounts, then long term liabilities would become immediately due, and the position of long term debtors would be called into question, resulting in the need to recognise that in the results presented in this set of accounts.
- Capital Expenditure
The amount expended by the trust that enhances the value of fixed assets whose useful life extends beyond the current accounting period.
- Revenue Expenditure
Expenditure on the day to day operations of the trust, pay and rations as opposed to capital expenditure.
- Consumables
Non pay expenditure on items that have a life of less than one year and are therefore not fixed assets. The term relates to everything from drugs, uniform, stationery through to pieces of disposable equipment.
- Integrated Care Systems (ICS)
ICSs have brought together commissioners of NHS services with health and care providers and other partners who work together to deliver services which meet the needs of specific populations. From 1 July 2022, Integrated Care Boards (ICB) became statutory bodies under the Health and Care Act 2022. ICBs have taken on the commissioning functions of CCGs as well as some of NHS England’s commissioning functions.
- Liability
A situation where an organisation has an obligation to pay for something that has already occurred, and around which there is certainty, but is not yet physically paid for.
- Provisions
An allowance in the accounts for a known item, but where the value or timing of the event giving rise to it is uncertain. An example may be where a pay award from 1 January in a given year has not yet been agreed, and the settlement date is uncertain. The organisation would typically provide an estimate for inclusion in the accounts to ensure that the relevant charge to Income and Expenditure is made in the correct year.
- Contingent Liability
A situation where a financial obligation to pay for something that has already happened may arise, but where there is uncertainty or where the final value is difficult to quantify due to dependencies on other things. For example, an outstanding legal claim against the organisation, where if the verdict goes against the organisation, there will be an obligation to pay for an unquantifiable amount. Amounts carried in the accounts under this heading will inevitably be estimates based on the best information available at the time.
- Value Added Tax (VAT)
May be in the form of output tax – VAT charged on sales, or input tax – VAT paid on purchases. In the NHS, normal NHS healthcare activity does not attract VAT.
- Post Balance Sheet Event
Something that is recognised after the accounts have been finalised, but before publication, which impacts on the results as they are presented, and has a significant impact on how the results should be interpreted.
- Risk Pooling Scheme
This is essentially the NHS insurance scheme, where we pay an annual premium to cover any insurance claims that may arise during the year. The scheme covers all the usual insurance risks around buildings, equipment, fire etc, as well as clinical negligence issues.
- NHS Resolution
NHS Resolution (NHSR) is the body responsible for handling negligence claims against NHS organisations. NHSR also advises NHS organisations on risk management.
- Losses and Special Payments
Any payments made in respect of bad debts, stock write offs, insurance excesses or compensation payments that are not considered a part of the normal business of the trust.
Things to consider when reading a set of accounts
- True and Fair View
A set of annual accounts is a snapshot at a point in time of how the business is performing. Is it profitable? Is it viable? Is it fit for purpose? It is not and probably never will be 100% accurate. What is important is that the accounts present a fair reflection of performance and viability, and that the items presented in there have been treated according valid and accepted accounting principles and can be explained and justified in that context.
- No Surprises
The annual accounts should only ever confirm what the board have been expecting in light of the monitoring reports that have been presented by the director of finance during the year and should bear a close resemblance to figures reported at month 12. If there are significant differences between what the board was expecting, or from the month 12 report, then the director of finance should include explanations for this in a commentary that accompanies the accounts, and the auditors should be asked to comment on any items of significance.
- Previous Year
It can be useful to compare this year’s figures with those of the previous year. Again, the board should already be aware of any significant movements, and the reasons for them, so any changes should be expected. If there are any changes that have not been explained, then these should be queried, and satisfactory explanations obtained to approval.
- Fixed Assets / Non-Current Assets
The board should be assured that the changes in the fixed asset figures from one year to another reflect the decisions made by the board on capital investment and disposals during the year. If a revaluation has taken place during the year, this should be explained in the notes, and the board should ensure that they are fully aware of the impact that this has had on both the Income and Expenditure account and balance sheet.
- Current Assets
Again, differences between years should be looked at. Particular things to look for include:
- Stock – large swings in stock levels year on year can indicate that stock management is inefficient. As a general rule, the trust should look to carry out as little stock as possible commensurate with ensuring that the right supplies are available at the right time. A very large reduction in stocks in any given year, combined with a reduction in cash balances, may be an indication that the trust is experiencing cash flow problems.
- Debtors – high levels of debtors may be a result of inefficient debt collection in the trust, and this may be impacting on the cash flow performance.
- Cash at bank and in hand – this is an indication of the liquidity of the trust. We should make sure that we have sufficient readily accessible cash available to meet our immediate needs. Significant swings from year to year may indicate that cash management is not as efficient as it should be.
Further Information
Contact the director of corporate affairs at the address, e-mail, or telephone number below for information about the board of directors or if you would like:
- To view the register of board of directors’ interests
- To contact the chair or any member of the board of directors
- Information about board of directors meetings which are open to the public. Details of meetings are also available on the trust’s website.
To contact the chief executive’s office for more information or if you have any comments
Write to: Director of Corporate Affairs
North West Ambulance Service NHS Trust
Ambulance Headquarters
Ladybridge Hall
Chorley New Road
Bolton
BL1 5DD
Telephone: 01204 498400
E-mail: [email protected]
Website: www.nwas.nhs.uk